Ridde Valéry, Agier Isabelle, Bonnet Emmanuel, Carabali Mabel, Dabiré Kounbobr Roch, Fournet Florence, Ly Antarou, Meda Ivlabèhiré Bertrand, Parra Beatriz
Department of Social and Preventive Medicine, University of Montreal School of Public Health (ESPUM), Montréal, Canada.
University of Montreal Public Health Research Institute (IRSPUM), Pavillon 7101 Avenue du Parc, P.O. Box 6128, Centre-ville Station, Montreal, Quebec, H3C 3J7, Canada.
Infect Dis Poverty. 2016 Apr 5;5:23. doi: 10.1186/s40249-016-0120-2.
The significant malaria burden in Africa has often eclipsed other febrile illnesses. Burkina Faso's first dengue epidemic occurred in 1925 and the most recent in 2013. Yet there is still very little known about dengue prevalence, its vector proliferation, and its poverty and equity impacts.
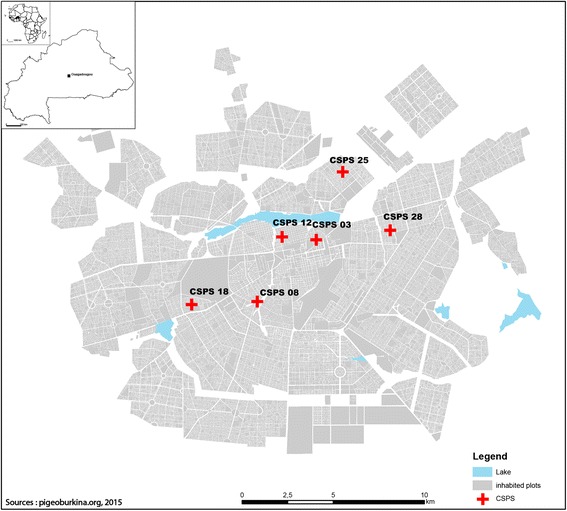
An exploratory cross-sectional survey was performed from December 2013 to January 2014. Six primary healthcare centers in Ouagadougou were selected based on previously reported presence of Flavivirus. All patients consulting with fever or having had fever within the previous week and with a negative rapid diagnostic test (RDT) for malaria were invited to participate. Sociodemographic data, healthcare use and expenses, mobility, health-related status, and vector control practices were captured using a questionnaire. Blood samples of every eligible subject were obtained through finger pricks during the survey for dengue RDT using SD BIOLINE Dengue Duo (NS1Ag and IgG/IgM)® and to obtain blood spots for reverse transcription polymerase chain reaction (RT-PCR) analysis. In a sample of randomly selected yards and those of patients, potential Aedes breeding sites were found and described. Larvae were collected and brought to the laboratory to monitor the emergence of adults and identify the species.
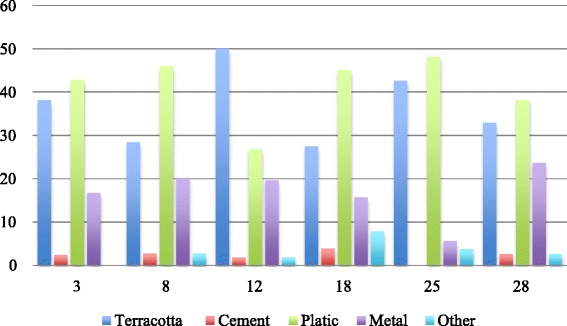
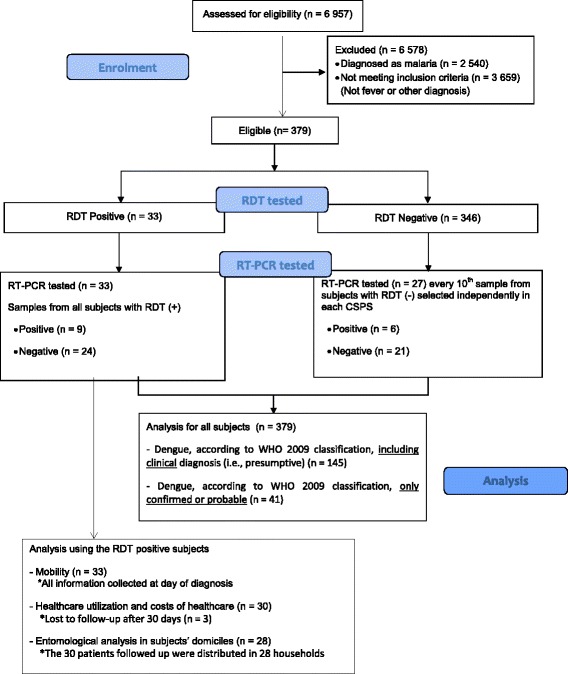
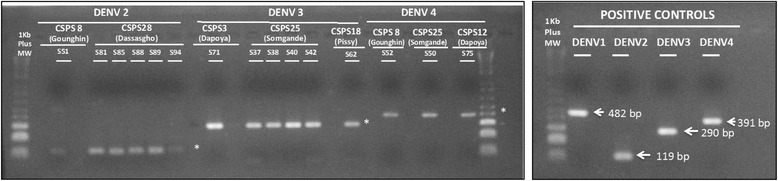
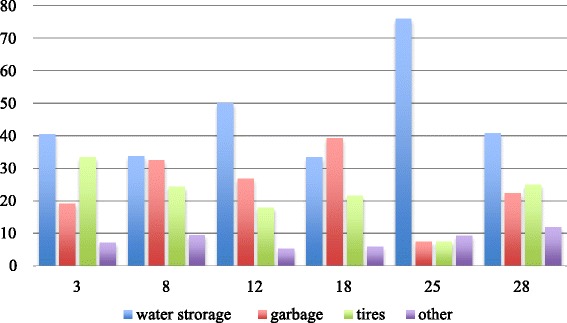
Of the 379 subjects, 8.7 % (33/379) had positive RDTs for dengue. Following the 2009 WHO classification, 38.3 % (145/379) had presumptive, probable, or confirmed dengue, based on either clinical symptoms or laboratory testing. Of 60 samples tested by RT-PCR (33 from the positive tests and 27 from the subsample of negatives), 15 were positive. The serotypes observed were DENV2, DENV3, and DENV4. Odds of dengue infection in 15-to-20-year-olds and persons over 50 years were 4.0 (CI 95 %: 1.0-15.6) and 7.7 (CI 95 %: 1.6-37.1) times higher, respectively, than in children under five. Average total spending for a dengue episode was 13 771 FCFA [1 300-67 300 FCFA] (1$US = 478 FCFA). On average, 2.6 breeding sites were found per yard. Potential Aedes breeding sites were found near 71.4 % (21/28) of patients, but no adult Aedes were found. The most frequently identified potential breeding sites were water storage containers (45.2 %). Most specimens collected in yards were Culex (97.9 %).
The scientific community, public health authorities, and health workers should consider dengue as a possible cause of febrile illness in Burkina Faso.
非洲严重的疟疾负担常常使其他发热性疾病黯然失色。布基纳法索的首次登革热疫情发生于1925年,最近一次是在2013年。然而,关于登革热的流行情况、其病媒繁殖以及对贫困和公平性的影响,人们仍然知之甚少。
2013年12月至2014年1月进行了一项探索性横断面调查。根据先前报告的黄病毒存在情况,在瓦加杜古选择了六个初级医疗保健中心。所有前来就诊的发热患者或前一周内曾发热且疟疾快速诊断检测(RDT)呈阴性的患者均被邀请参与。通过问卷调查收集社会人口学数据、医疗保健使用情况和费用、流动性、健康相关状况以及病媒控制措施。在调查期间,通过手指针刺采集每个符合条件的受试者的血样,使用SD BIOLINE登革热双联检测试剂(NS1抗原和IgG/IgM)进行登革热RDT检测,并获取血斑用于逆转录聚合酶链反应(RT-PCR)分析。在随机选择的院子和患者的院子中,发现并描述了潜在的伊蚊繁殖地。收集幼虫并带回实验室,以监测成虫的出现并鉴定物种。
在379名受试者中,8.7%(33/379)的登革热RDT检测呈阳性。根据2009年世界卫生组织的分类,基于临床症状或实验室检测,38.3%(145/379)的患者患有疑似、可能或确诊的登革热。在通过RT-PCR检测的60个样本中(33个来自阳性检测,27个来自阴性子样本),15个呈阳性。观察到的血清型为DENV2、DENV3和DENV4。15至20岁人群和50岁以上人群感染登革热的几率分别比5岁以下儿童高4.0倍(95%置信区间:1.0 - 15.6)和7.7倍(95%置信区间:1.6 - 37.1)。登革热发作的平均总花费为13771非洲法郎[1300 - 67300非洲法郎](1美元 = 478非洲法郎)。每个院子平均发现2.6个繁殖地。在71.4%(21/28)的患者附近发现了潜在的伊蚊繁殖地,但未发现成年伊蚊。最常发现的潜在繁殖地是储水容器(45.2%)。在院子里收集的大多数标本是库蚊(97.9%)。
科学界、公共卫生当局和卫生工作者应将登革热视为布基纳法索发热性疾病的可能病因。