Toutous Trellu Laurence, Nkemenang Patrick, Comte Eric, Ehounou Geneviève, Atangana Paul, Mboua Didier Junior, Rusch Barbara, Njih Tabah Earnest, Etard Jean-François, Mueller Yolanda K
Geneva University Hospitals, Geneva, Switzerland.
Médecins Sans Frontières, Geneva, Switzerland.
PLoS Negl Trop Dis. 2016 Apr 13;10(4):e0004385. doi: 10.1371/journal.pntd.0004385. eCollection 2016 Apr.
Clinical diagnosis of Buruli ulcer (BU) due to Mycobacterium ulcerans can be challenging. We aimed to specify the differential diagnosis of skin lesions in a BU endemic area.
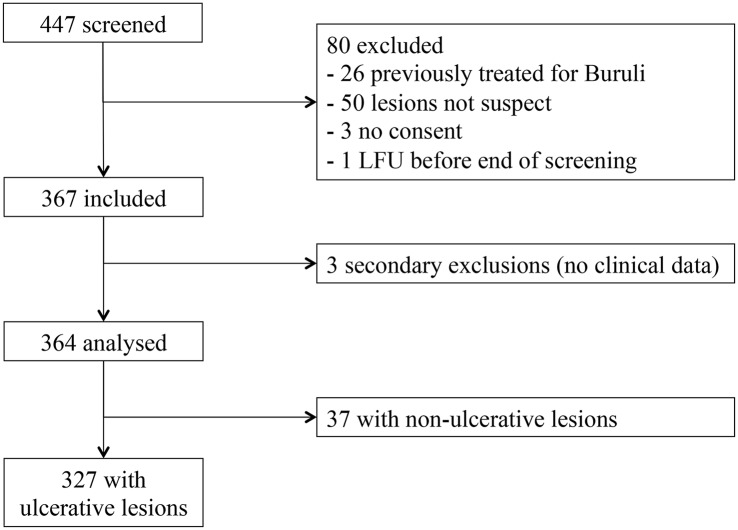
We conducted a prospective diagnostic study in Akonolinga, Cameroon. Patients presenting with a skin ulcer suspect of BU were included. M. ulcerans was detected using swabs for Ziehl-Neelsen staining, PCR and culture. Skin punch biopsies were taken and reviewed by two histopathologists. Photographs of the lesions were taken and independently reviewed by two dermatologists. Final diagnosis was based on consensus, combining the results of laboratory tests and expert opinion.
RESULTS/ DISCUSSION: Between October 2011 and December 2013, 327 patients with ulcerative lesions were included. Median age was 37 years (0 to 87), 65% were males, and 19% HIV-positive. BU was considered the final diagnosis for 27% of the lesions, 85% of which had at least one positive laboratory test. Differential diagnoses were vascular lesions (22%), bacterial infections (21%), post-traumatic (8%), fistulated osteomyelitis (6%), neoplasia (5%), inflammatory lesions (3%), hemopathies and other systemic diseases (2%) and others (2%). The proportion of BU was similar between HIV-positive and HIV-negative patients (27.0% vs. 26.5%; p = 0.940). Half of children below 15 years of age were diagnosed with BU, compared to 26.8% and 13.9% among individuals 15 to 44 years of age and above, respectively (chi2 p<0.001). Children had more superficial bacterial infections (24.3%) and osteomyelitis (11.4%).
We described differential diagnosis of skin lesions in a BU endemic area, stratifying results by age and HIV-status.
由溃疡分枝杆菌引起的布鲁里溃疡(BU)的临床诊断可能具有挑战性。我们旨在明确布鲁里溃疡流行地区皮肤病变的鉴别诊断。
我们在喀麦隆的阿科诺林加进行了一项前瞻性诊断研究。纳入出现疑似布鲁里溃疡皮肤溃疡的患者。使用拭子进行萋尼氏染色、聚合酶链反应(PCR)和培养以检测溃疡分枝杆菌。采集皮肤打孔活检标本并由两名组织病理学家进行检查。拍摄病变照片并由两名皮肤科医生独立检查。最终诊断基于综合实验室检查结果和专家意见达成的共识。
结果/讨论:2011年10月至2013年12月期间,纳入了327例溃疡性病变患者。中位年龄为37岁(0至87岁),65%为男性,19%为HIV阳性。27%的病变最终诊断为布鲁里溃疡,其中85%至少有一项实验室检查呈阳性。鉴别诊断包括血管性病变(22%)、细菌感染(21%)、创伤后病变(8%)、瘘管性骨髓炎(6%)、肿瘤(5%)、炎性病变(3%)、血液病和其他全身性疾病(2%)以及其他(2%)。HIV阳性和HIV阴性患者中布鲁里溃疡的比例相似(27.0%对26.5%;p = 0.940)。15岁以下儿童中有一半被诊断为布鲁里溃疡,而15至44岁及以上个体中的比例分别为26.8%和13.9%(卡方检验p<0.001)。儿童浅表细菌感染(24.3%)和骨髓炎(11.4%)更多。
我们描述了布鲁里溃疡流行地区皮肤病变的鉴别诊断,并按年龄和HIV感染状况对结果进行了分层。