Fitzgerald Rhys, Owen Rebecca, Barry Tamara, Hargrave Cathy, Pryor David, Bernard Anne, Lehman Margot, Mai Tao, Fielding Andrew
Division of Radiation Therapy Princess Alexandra Hospital Woolloongabba Queensland Australia; Science and Engineering Faculty Queensland University of Technology Brisbane Queensland Australia.
Radiation Oncology Mater Centre South Brisbane Queensland Australia.
J Med Radiat Sci. 2016 Mar;63(1):31-40. doi: 10.1002/jmrs.118. Epub 2015 Jul 14.
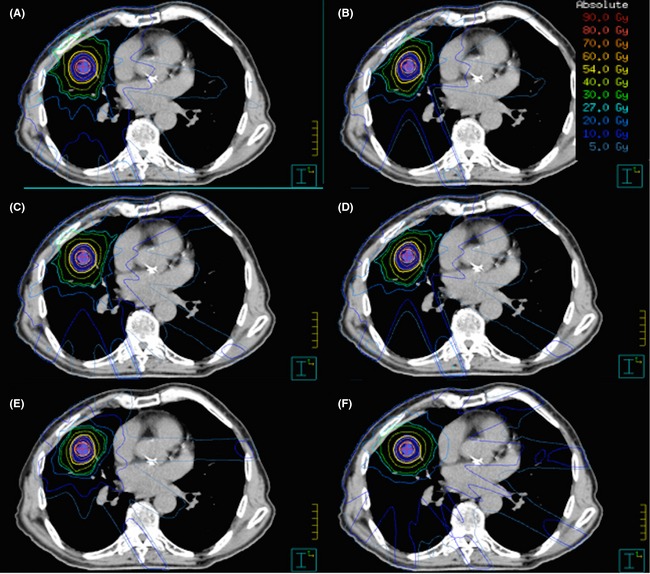
The aim of this study was to compare various coplanar and non-coplanar 3-dimensional conformal radiation therapy (3DCRT) beam arrangements for the delivery of stereotactic ablative radiation therapy (SABR) to patients with early stage lung cancer, based on the dosimetric criteria from the Radiation Therapy Oncology Group (RTOG) 1021 protocol.
Ten medically inoperable lung cancer patients eligible for SABR were re-planned using three different coplanar and three different non-coplanar beam arrangements. The plans were compared by assessing planning target volume (PTV) coverage, doses to normal tissues, the high-dose conformity (conformity index) and intermediate dose spillage as defined by the D2cm, (the dose at any point 2 cm away from the PTV), and the R50% (the ratio of the volume of half the prescription dose to the volume of the PTV).
Sixty plans in total were assessed. Mean PTV coverage with the prescription isodose was similar between coplanar (95.14%) and non-coplanar (95.26%) techniques (P = 0.47). There was significant difference between all coplanar and all non-coplanar fields for the R50% (P < 0.0001) but none for the D2cm (P = 0.19). The seven and nine field beam arrangements with two non-coplanar fields had less unacceptable protocol deviations (10 and 7) than the seven and nine field plans with only coplanar fields (13 and 8). The 13 field coplanar fields did not improve protocol compliance with eight unacceptable deviations. The 10 field non-coplanar beam arrangement achieved best compliance with the RTOG 1021 dose criteria with only one unacceptable deviation (maximum rib dose).
A 3DCRT planning technique using 10 fields with ≥6 non-coplanar beams best satisfied high and intermediate dose constraints stipulated in the RTOG 1021 trial. Further investigations are required to determine if minor protocol deviations should be balanced against efficiency with the extended treatment times required to deliver non-coplanar fields and if treatment times can be improved using novel intensity modulated techniques.
本研究的目的是根据放射治疗肿瘤学组(RTOG)1021方案的剂量学标准,比较各种共面和非共面三维适形放射治疗(3DCRT)射束排列用于早期肺癌患者立体定向消融放疗(SABR)的情况。
对10例符合SABR条件的医学上无法手术的肺癌患者,使用三种不同的共面和三种不同的非共面射束排列重新进行计划。通过评估计划靶体积(PTV)覆盖情况、正常组织剂量、高剂量适形性(适形指数)以及如D2cm(距PTV任何点2 cm处的剂量)和R50%(处方剂量一半的体积与PTV体积之比)所定义的中间剂量溢出,对这些计划进行比较。
总共评估了60个计划。共面(95.14%)和非共面(95.26%)技术的处方等剂量线的平均PTV覆盖情况相似(P = 0.47)。所有共面和所有非共面射野的R50%存在显著差异(P < 0.0001),但D2cm无显著差异(P = 0.19)。具有两个非共面射野的七野和九野射束排列的不可接受方案偏差(分别为10和7)比仅具有共面射野的七野和九野计划(分别为13和8)少。13野共面射野并未改善方案依从性,有八个不可接受偏差。10野非共面射束排列对RTOG 1021剂量标准的依从性最佳,只有一个不可接受偏差(最大肋骨剂量)。
使用10个射野且≥6个非共面射束的3DCRT计划技术最能满足RTOG 1021试验规定的高剂量和中间剂量限制。需要进一步研究以确定较小的方案偏差是否应与非共面射野所需延长治疗时间的效率相权衡,以及是否可以使用新型调强技术改善治疗时间。