Jin Chen, Li Wei, Qiao Shu-Bin, Yang Jin-Gang, Wang Yang, He Pei-Yuan, Tang Xin-Ran, Dong Qiu-Ting, Li Xiang-Dong, Yan Hong-Bing, Wu Yong-Jian, Chen Ji-Lin, Gao Run-Lin, Yuan Jin-Qing, Dou Ke-Fei, Xu Bo, Zhao Wei, Zhang Xue, Xian Ying, Yang Yue-Jin
State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
J Am Heart Assoc. 2016 Apr 22;5(4):e002684. doi: 10.1161/JAHA.115.002684.
Transradial percutaneous coronary intervention (PCI) has been increasingly adopted in clinical practice, given its potential advantages over transfemoral intervention; however, the impact of different access strategies on costs and clinical outcomes remains poorly defined, especially in the developing world.
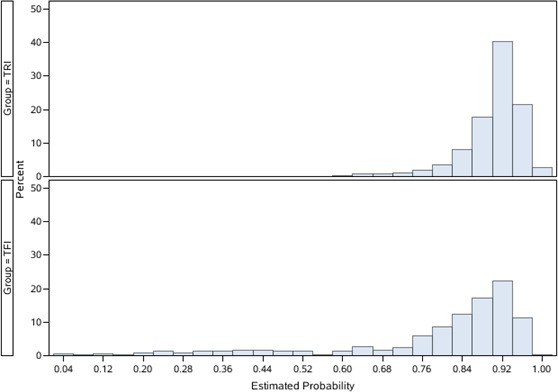
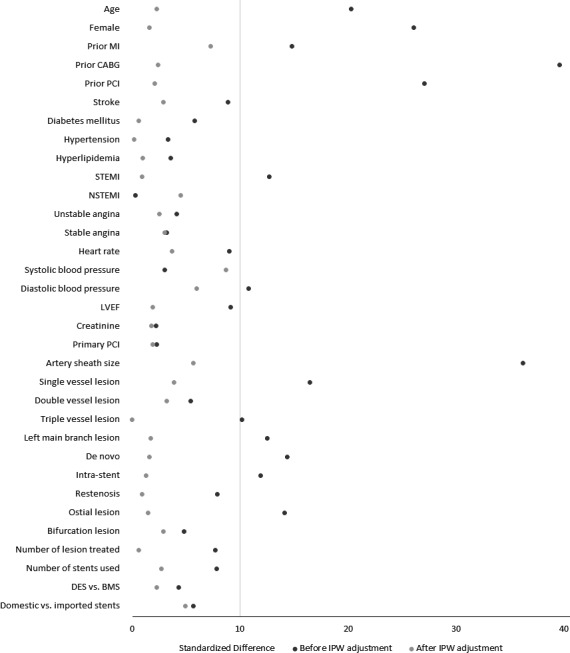
Using data from a consecutive cohort of 5306 patients undergoing PCI in China in 2010, we compared total hospital costs and in-hospital outcomes for transradial intervention (TRI) and transfemoral intervention. Patients receiving TRI (n=4696, 88.5%) were slightly younger (mean age 57.4 versus 59.5 years), less often women (21.6% versus 33.1%), more likely to undergo PCI for single-vessel disease, and less likely to undergo PCI for triple-vessel or left main diseases. The unadjusted total hospital costs were 57 900 Chinese yuan (¥57 900; equivalent to 9190 US dollars [$9190]) for TRI and ¥67 418 ($10,701) for transfemoral intervention. After adjusting for all observed patient and procedural characteristics using the propensity score inverse probability weighting method, TRI was associated with a lower total cost (adjusted difference ¥8081 [$1283]). More than 80% of the cost difference was related to lower PCI-related costs (adjusted difference -¥5162 [-$819]), which were likely driven by exclusive use of vascular closure devices in transfemoral intervention, and lower hospitalization costs (-¥1399 [-$222]). Patients receiving TRI had shorter length of stay and were less likely to experience major adverse cardiac events or post-PCI bleeding. These differences were consistent among clinically relevant subgroups with acute myocardial infarction, acute coronary syndrome, and stable angina.
Among patients undergoing PCI, TRI was associated with lower cost and favorable clinical outcomes compared with transfemoral intervention.
经桡动脉冠状动脉介入治疗(PCI)因其相较于经股动脉介入治疗具有潜在优势,已在临床实践中得到越来越广泛的应用;然而,不同入路策略对成本和临床结局的影响仍未明确,尤其是在发展中国家。
利用2010年在中国连续入选的5306例行PCI患者的数据,我们比较了经桡动脉介入治疗(TRI)和经股动脉介入治疗的总住院费用及住院期间结局。接受TRI的患者(n = 4696,88.5%)年龄稍小(平均年龄57.4岁对59.5岁),女性比例较低(21.6%对33.1%),单支血管病变行PCI的可能性更大,三支血管或左主干病变行PCI的可能性更小。未调整的总住院费用TRI为57 900元人民币(57 900元;相当于9190美元),经股动脉介入治疗为67 418元(10 701美元)。使用倾向评分逆概率加权法对所有观察到的患者和手术特征进行调整后,TRI与较低的总成本相关(调整后差异8081元[1283美元])。超过80%的成本差异与较低的PCI相关成本(调整后差异 - 5162元[- 819美元])有关,这可能是由于经股动脉介入治疗中血管闭合装置的独家使用以及较低的住院费用(- 1399元[- 222美元])所致。接受TRI的患者住院时间较短,发生主要不良心脏事件或PCI术后出血的可能性较小。这些差异在急性心肌梗死、急性冠状动脉综合征和稳定型心绞痛等临床相关亚组中是一致的。
在接受PCI的患者中,与经股动脉介入治疗相比,TRI与较低的成本和良好的临床结局相关。