Swim Across America Laboratory, Immunology Program, Sloan-Kettering Institute for Cancer Research, New York, New York, USA; Department of Medicine, Gynecologic Medical Oncology Service, Memorial Sloan Kettering Cancer Center, New York, New York, USA; Ludwig Center for Cancer Immunotherapy at Memorial Sloan-Kettering Cancer Center, New York, New York, USA; Weill Cornell Medical College and Graduate School of Medical Sciences of Cornell University, New York, New York, USA.
Swim Across America Laboratory, Immunology Program, Sloan-Kettering Institute for Cancer Research, New York, New York, USA; Department of Medicine, Melanoma and Immunotherapy Service, Memorial Sloan Kettering Cancer Center, New York, New York, USA; Ludwig Center for Cancer Immunotherapy at Memorial Sloan-Kettering Cancer Center, New York, New York, USA; Weill Cornell Medical College and Graduate School of Medical Sciences of Cornell University, New York, New York, USA.
Mol Ther Oncolytics. 2014 Dec 10;1:14004. doi: 10.1038/mto.2014.4. eCollection 2014.
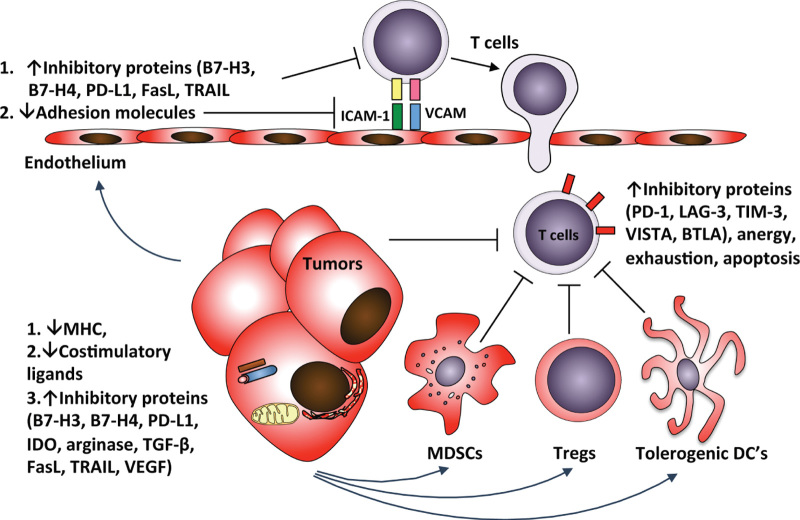
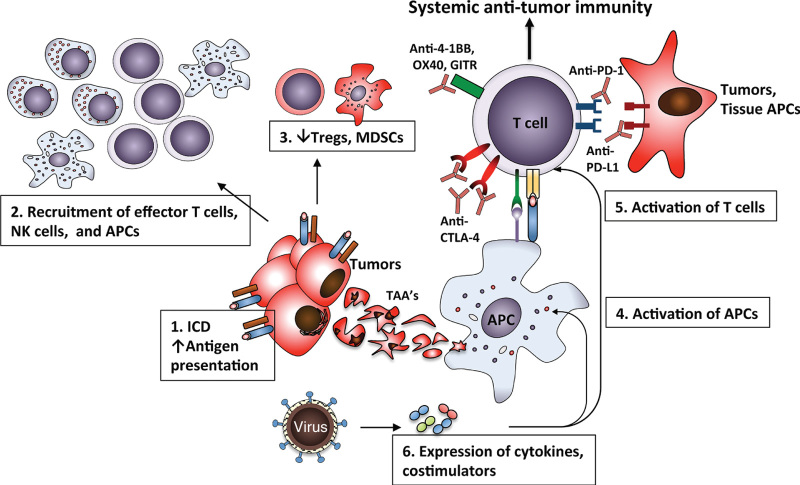
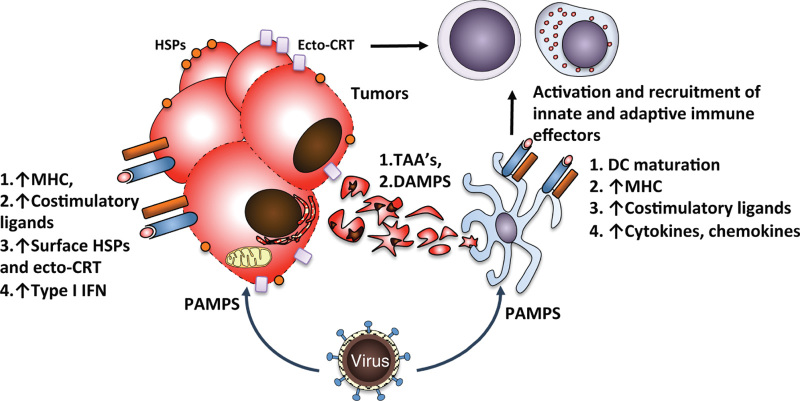
Identification of the immune suppressive mechanisms active within the tumor microenvironment led to development of immunotherapeutic strategies aiming to reverse the immunosuppression and to enhance the function of tumor-infiltrating lymphocytes. Of those, cancer therapy with antibodies targeting the immune costimulatory and coinhibitory receptors has demonstrated significant promise in the recent years, with multiple antibodies entering clinical testing. The responses to these agents, however, have not been universal and have not been observed in all cancer types, calling for identification of appropriate predictive biomarkers and development of combinatorial strategies. Pre-existing immune infiltration in tumors has been demonstrated to have a strong association with response to immunotherapies, with the type I interferon (IFN) pathway emerging as a key player in tumor innate immune recognition and activation of adaptive immunity. These findings provide a rationale for evaluation of strategies targeting the type I IFN pathway as a means to enhance tumor immune recognition and infiltration, which could potentially make them susceptible to therapeutics targeting the cosignaling receptors. To this end in particular, oncolytic viruses (OVs) have been demonstrated to enhance tumor recognition by the immune system through multiple mechanisms, which include upregulation of major histocompatibility complex and costimulatory molecules on cancer cells, immunogenic cell death and antigen release, and activation of the type I IFN pathway. Evidence is now emerging that combination therapies using OVs and agents targeting immune cosignaling receptors such as 4-1BB, PD-1, and CTLA-4 may work in concert to enhance antitumor immunity and therapeutic efficacy. Our evolving understanding of the interplay between OVs and the immune system demonstrates that the virus-induced antitumor immune responses can be harnessed to drive the efficacy of the agents targeting cosignaling receptors and provides a strong rationale for integration of such therapies in clinic.
鉴定肿瘤微环境中具有免疫抑制作用的机制,导致了免疫治疗策略的发展,旨在逆转免疫抑制,增强肿瘤浸润淋巴细胞的功能。近年来,针对免疫共刺激和共抑制受体的癌症治疗抗体显示出了显著的前景,多种抗体已进入临床测试。然而,这些药物的反应并非普遍存在,也并非在所有癌症类型中都观察到,这需要确定合适的预测生物标志物并开发联合策略。已经证明,肿瘤中预先存在的免疫浸润与对免疫治疗的反应密切相关,其中 I 型干扰素(IFN)途径成为肿瘤固有免疫识别和适应性免疫激活的关键因素。这些发现为评估靶向 I 型 IFN 途径的策略提供了依据,这些策略可能增强肿瘤免疫识别和浸润,从而使其对靶向共信号受体的治疗药物敏感。为此,溶瘤病毒(OVs)已被证明通过多种机制增强免疫系统对肿瘤的识别,包括上调癌细胞上的主要组织相容性复合体和共刺激分子、免疫原性细胞死亡和抗原释放以及激活 I 型 IFN 途径。现在有证据表明,OVs 与靶向免疫共信号受体(如 4-1BB、PD-1 和 CTLA-4)的联合治疗可能协同作用,增强抗肿瘤免疫和治疗效果。我们对 OVs 与免疫系统之间相互作用的不断深入的理解表明,病毒诱导的抗肿瘤免疫反应可以被利用来增强靶向共信号受体的药物的疗效,并为将这些疗法整合到临床中提供了强有力的理由。