Hamrefors Viktor, Härstedt Maria, Holmberg Anna, Rogmark Cecilia, Sutton Richard, Melander Olle, Fedorowski Artur
Department of Clinical Sciences, Faculty of Medicine, Lund University, Malmö, Sweden.
Department of Medical Imaging and Physiology, Skåne University Hospital, Malmö, Sweden.
PLoS One. 2016 Apr 28;11(4):e0154249. doi: 10.1371/journal.pone.0154249. eCollection 2016.
Autonomic disorders of the cardiovascular system, such as orthostatic hypotension and elevated resting heart rate, predict mortality and cardiovascular events in the population. Low-energy-fractures constitute a substantial clinical problem that may represent an additional risk related to such autonomic dysfunction.
To test the association between orthostatic hypotension, resting heart rate and incidence of low-energy-fractures in the general population.
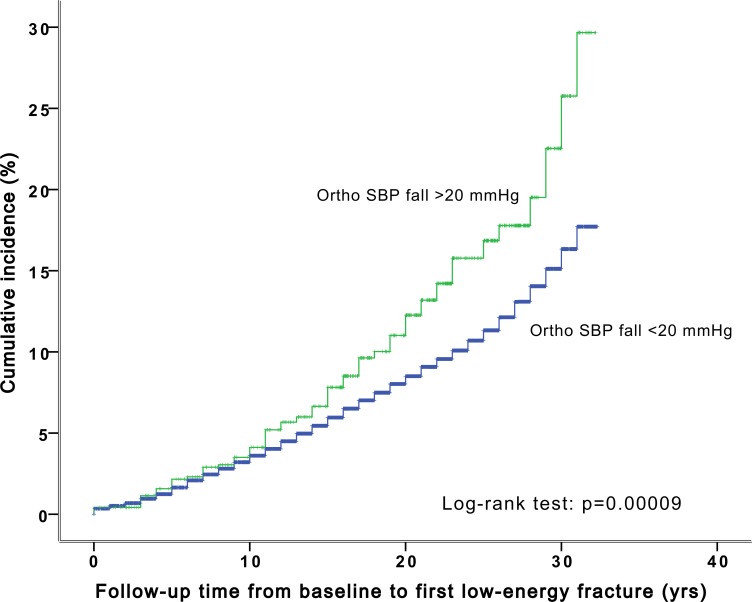
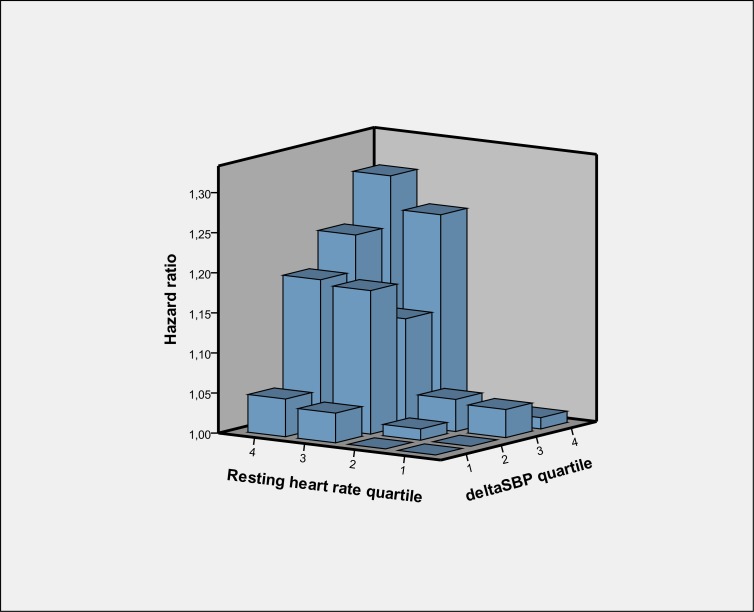
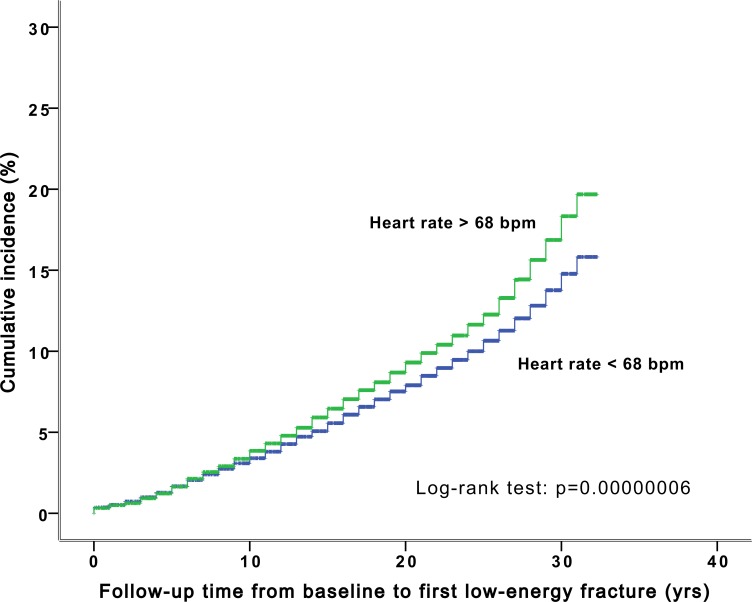
Using multivariable-adjusted Cox regression models we investigated the association between orthostatic blood pressure response, resting heart rate and first incident low-energy-fracture in a population-based, middle-aged cohort of 33 000 individuals over 25 years follow-up. The median follow-up time from baseline to first incident fracture among the subjects that experienced a low energy fracture was 15.0 years. A 10 mmHg orthostatic decrease in systolic blood pressure at baseline was associated with 5% increased risk of low-energy-fractures (95% confidence interval 1.01-1.10) during follow-up, whereas the resting heart rate predicted low-energy-fractures with an effect size of 8% increased risk per 10 beats-per-minute (1.05-1.12), independently of the orthostatic response. Subjects with a resting heart rate exceeding 68 beats-per-minute had 18% (1.10-1.26) increased risk of low-energy-fractures during follow-up compared with subjects with a resting heart rate below 68 beats-per-minute. When combining the orthostatic response and resting heart rate, there was a 30% risk increase (1.08-1.57) of low-energy-fractures between the extremes, i.e. between subjects in the fourth compared with the first quartiles of both resting heart rate and systolic blood pressure-decrease.
Orthostatic blood pressure decline and elevated resting heart rate independently predict low-energy fractures in a middle-aged population. These two measures of subclinical cardiovascular dysautonomia may herald increased risks many years in advance, even if symptoms may not be detectable. Although the effect sizes are moderate, the easily accessible clinical parameters of orthostatic blood pressure response and resting heart rate deserve consideration as new risk predictors to yield more accurate decisions on primary prevention of low-energy fractures.
心血管系统的自主神经功能紊乱,如体位性低血压和静息心率升高,可预测人群中的死亡率和心血管事件。低能量骨折是一个重大的临床问题,可能代表着与这种自主神经功能障碍相关的额外风险。
检验体位性低血压、静息心率与普通人群中低能量骨折发生率之间的关联。
我们使用多变量调整的Cox回归模型,在一个基于人群的、33000名中年人的队列中,对其进行超过25年的随访,研究体位性血压反应、静息心率与首次发生低能量骨折之间的关联。经历低能量骨折的受试者从基线到首次发生骨折的中位随访时间为15.0年。基线时收缩压体位性下降10 mmHg与随访期间低能量骨折风险增加5%相关(95%置信区间1.01 - 1.10),而静息心率预测低能量骨折的效应大小为每10次/分钟增加8%的风险(1.05 - 1.12),与体位性反应无关。静息心率超过68次/分钟的受试者在随访期间发生低能量骨折的风险比静息心率低于68次/分钟的受试者高18%(1.10 - 1.26)。当结合体位性反应和静息心率时,在两个极端情况之间,即静息心率和收缩压下降处于第四四分位数与第一四分位数的受试者之间,低能量骨折的风险增加30%(1.08 - 1.57)。
体位性血压下降和静息心率升高独立预测中年人群中的低能量骨折。这两种亚临床心血管自主神经功能障碍的指标可能在许多年前就预示着风险增加,即使症状可能无法检测到。尽管效应大小适中,但体位性血压反应和静息心率这些易于获取的临床参数值得作为新的风险预测指标加以考虑,以便在低能量骨折的一级预防中做出更准确的决策。