Na Hyo-Seok, Oh Ah-Young, Koo Bon-Wook, Lim Dae-Jin, Ryu Jung-Hee, Han Ji-Won
From the Department of Anesthesiology and Pain Medicine, Seoul National University Bundang Hospital, Seongnam (H-SN, A-YO, B-WK, J-HR, J-WH); Department of Anesthesiology and Pain Medicine, Yonsei Barun Orthopedic Clinic, Yongin (D-JL), Gyeonggi; and Department of Anesthesiology and Pain Medicine, Seoul National University College of Medicine, Seoul (A-YO, J-HR), Republic of Korea.
Medicine (Baltimore). 2016 May;95(20):e3705. doi: 10.1097/MD.0000000000003705.
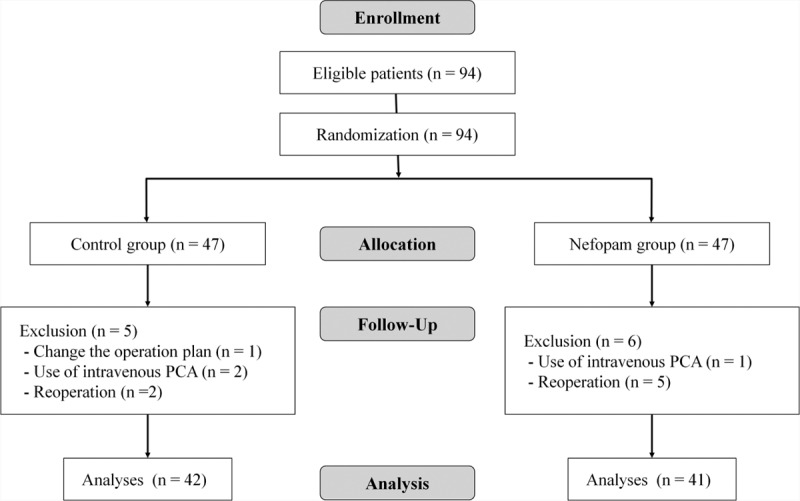
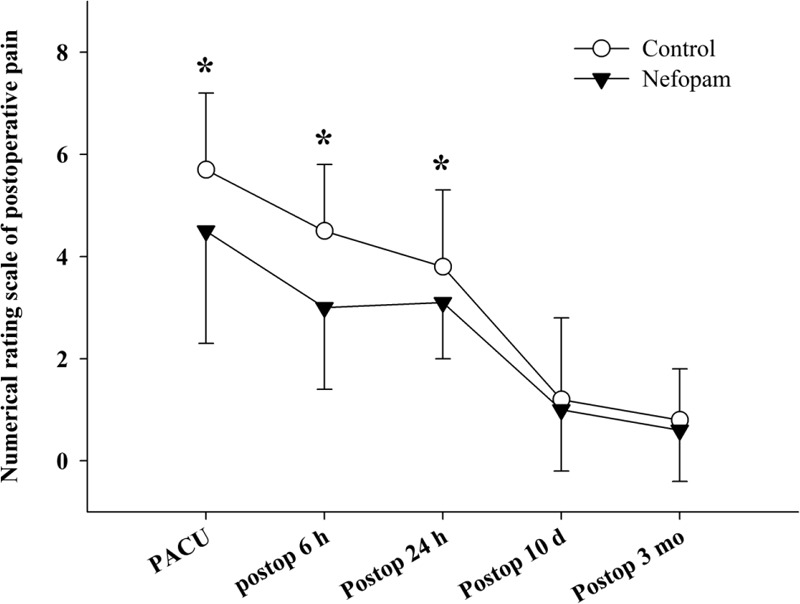
Breast cancer surgery is known to cause severe acute postoperative pain, which can persist for a long time. We administered nefopam preventively to patients undergoing lumpectomy with axillary lymph node dissection or sentinel lymph node biopsy, and evaluated its efficacy on acute and chronic postoperative pain.Enrolled patients were assigned to the nefopam (n = 41) or the control (n = 42) group. Before initiating the operation, 20 mg of nefopam was given to the patients of the nefopam group, and normal saline was used in the control group. Ketorolac was given at the end of surgery, and meloxicam was prescribed in the postoperative period to all patients in both groups. Pain was assessed using a numerical rating scale (NRS), and the rescue analgesic drug was given when the NRS was >5. Implementation of postoperative chemotherapy, radiotherapy (RT), or hormone therapy was evaluated.The NRS of postoperative pain was significantly lower in the nefopam than in the control group in the postanesthetic care unit (4.5 ± 2.2 vs 5.7 ± 1.5, respectively; P = 0.01), at postoperative 6 h (3.0 ± 1.6 vs 4.5 ± 1.3, respectively; P < 0.001), and at postoperative 24 h (3.1 ± 1.1 vs 3.8 ± 1.5, respectively; P = 0.01) with reduced use of rescue analgesic drugs. Significantly fewer patients suffered from chronic postoperative pain in the nefopam than in the control group at postoperative 3 months (36.6% vs 59.5%, P = 0.04). Considering only the cohort without postoperative adjuvant RT, the difference in the proportion of patients reporting chronic pain increased (23.5% in the nefopam group vs 61.5% in the control group, P = 0.04).Preventive nefopam was helpful in reducing the acute postoperative pain, with reduced use of rescue analgesic drugs, and it contributed to reduced occurrence of chronic pain at postoperative 3 months after breast cancer surgery.
乳腺癌手术会导致严重的术后急性疼痛,且这种疼痛可能会持续很长时间。我们对接受保乳手术并腋窝淋巴结清扫或前哨淋巴结活检的患者预防性给予奈福泮,并评估其对术后急性和慢性疼痛的疗效。纳入的患者被分配到奈福泮组(n = 41)或对照组(n = 42)。在手术开始前,给奈福泮组患者给予20mg奈福泮,对照组使用生理盐水。手术结束时给予酮咯酸,术后两组所有患者均开具美洛昔康。使用数字评分量表(NRS)评估疼痛,当NRS>5时给予解救镇痛药。评估术后化疗、放疗(RT)或激素治疗的实施情况。在麻醉后护理单元,奈福泮组术后疼痛的NRS显著低于对照组(分别为4.5±2.2和5.7±1.5;P = 0.01),术后6小时(分别为3.0±1.6和4.5±1.3;P < 0.001),以及术后24小时(分别为3.1±1.1和3.8±1.5;P = 0.01),同时解救镇痛药的使用减少。术后3个月,奈福泮组慢性术后疼痛的患者明显少于对照组(36.6%对59.5%,P = 0.04)。仅考虑无术后辅助放疗的队列,报告慢性疼痛的患者比例差异增大(奈福泮组为23.5%,对照组为61.5%,P = 0.04)。预防性给予奈福泮有助于减轻术后急性疼痛,减少解救镇痛药的使用,并有助于降低乳腺癌手术后3个月慢性疼痛的发生率。