University of Texas Health Science Center at San Antonio, San Antonio, TX, USA; San Antonio Military Medical Center, San Antonio, TX, USA.
University of Texas Health Science Center at San Antonio , San Antonio, TX , USA.
Front Pediatr. 2016 May 6;4:42. doi: 10.3389/fped.2016.00042. eCollection 2016.
To correlate sonographic renal parenchymal measurements among patients with ureteropelvic junction obstruction (UPJO) labeled society of fetal urology (SFU) hydronephrosis grades 1-4 and to examine whether sonographic renal parenchymal measurements could be used to differentiate conservative vs. surgical management.
Retrospective chart review and sonographic renal parenchymal measurements (renal length, medullary pyramid thickness, and renal parenchymal thickness) were performed in patients with SFU grades 1-4 hydronephrosis secondary to UPJO managed between 2009 and 2014. Exclusion criteria included other concomitant genitourinary pathology or incomplete follow-up. Anterior-posterior renal pelvic diameter (APRPD) and radionuclide renography were also evaluated when available.
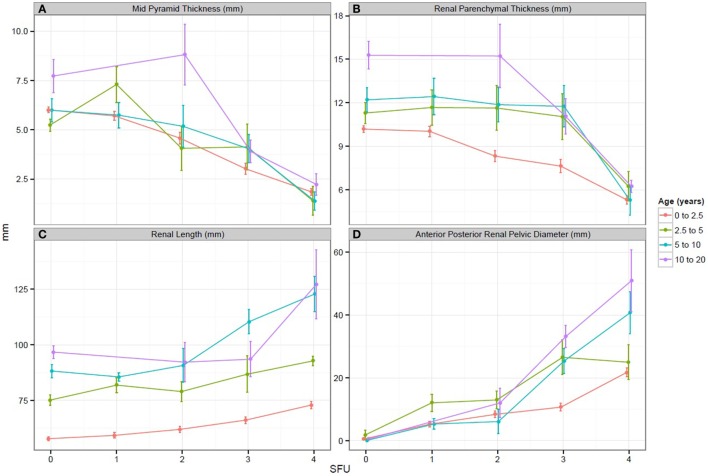
One hundred four patients with UPJO underwent 244 renal and bladder ultrasound (1,464 sonographic renal parenchymal measurements in 488 kidneys). Medullary pyramid thickness and renal parenchymal thickness progressively decreased from SFU grades 1-4 (p < 0.05). A similar trend was appreciated when comparing SFU grades 1 and 2 vs. 3 and 4, as well as SFU grades 3 vs. 4 (p < 0.05). SFU grade 3 and 4 patients who underwent pyeloplasty had longer renal length in comparison to those who were managed conservatively (p < 0.02).
This is the first study that evaluates these objective, quantifiable sonographic renal parenchymal measurements in children with unilateral UPJO. These sonographic renal parenchymal measurements correlate closely with worsening of hydronephrosis graded by the SFU and APRPD classification systems. Prospective studies are needed to elucidate the role of sonographic renal parenchymal measurements in the management of children with UPJO.
分析胎儿泌尿外科学会(SFU)分级 1-4 级积水的肾盂输尿管连接部梗阻(UPJO)患者的肾脏实质超声测量值,并探讨超声肾脏实质测量值是否可用于区分保守治疗与手术治疗。
回顾性分析 2009 年至 2014 年间接受治疗的 SFU 分级 1-4 级积水的 UPJO 患者的病历和超声肾脏实质测量值(肾长度、肾髓质锥体厚度和肾实质厚度)。排除标准包括其他伴发的泌尿生殖系统病变或随访不完整。当有条件时,还评估了前后肾盂直径(APRPD)和放射性核素肾图。
104 例 UPJO 患者接受了 244 次肾脏和膀胱超声检查(488 个肾脏的 1464 次超声肾脏实质测量)。肾髓质锥体厚度和肾实质厚度从 SFU 分级 1-4 逐渐降低(p<0.05)。当比较 SFU 分级 1 和 2 与 3 和 4 时,以及 SFU 分级 3 与 4 时,也观察到了类似的趋势(p<0.05)。与保守治疗相比,接受肾盂成形术的 SFU 分级 3 和 4 患者的肾长度更长(p<0.02)。
这是第一项评估单侧 UPJO 儿童这些客观、可量化的超声肾脏实质测量值的研究。这些超声肾脏实质测量值与 SFU 和 APRPD 分类系统分级的积水严重程度密切相关。需要前瞻性研究来阐明超声肾脏实质测量值在 UPJO 患儿管理中的作用。