Jenkins Kathy J, Koch Kupiec Jennifer, Owens Pamela L, Romano Patrick S, Geppert Jeffrey J, Gauvreau Kimberlee
Boston Children's Hospital, Boston, MA
Boston Children's Hospital, Boston, MA.
J Am Heart Assoc. 2016 May 20;5(5):e003028. doi: 10.1161/JAHA.115.003028.
The National Quality Forum previously approved a quality indicator for mortality after congenital heart surgery developed by the Agency for Healthcare Research and Quality (AHRQ). Several parameters of the validated Risk Adjustment for Congenital Heart Surgery (RACHS-1) method were included, but others differed. As part of the National Quality Forum endorsement maintenance process, developers were asked to harmonize the 2 methodologies.
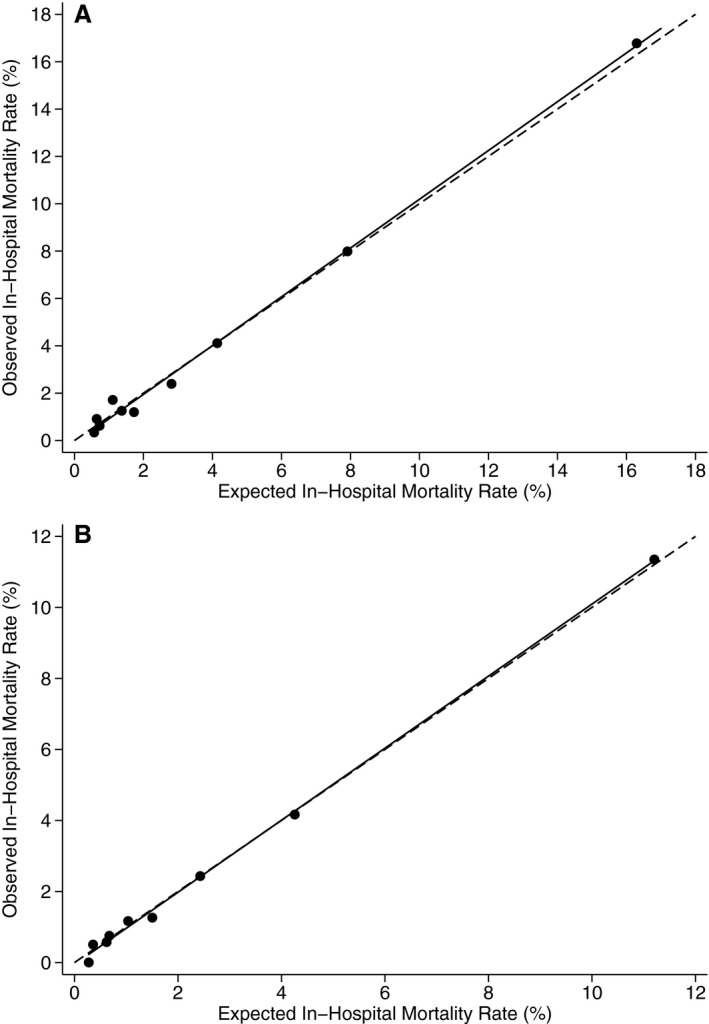
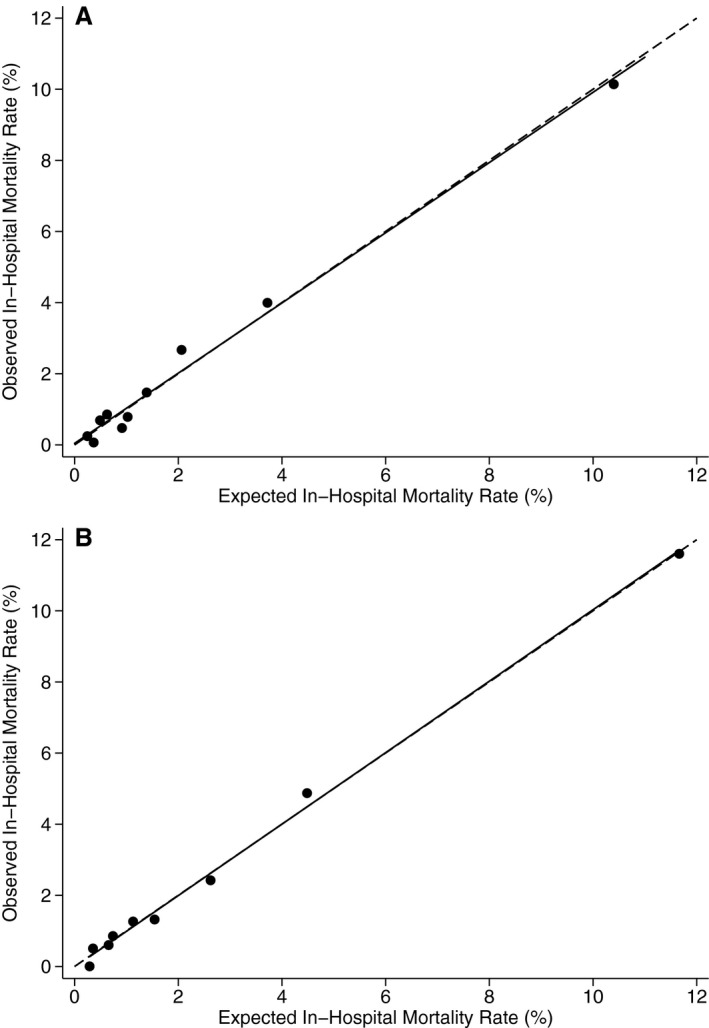
Parameters that were identical between the 2 methods were retained. AHRQ's Healthcare Cost and Utilization Project State Inpatient Databases (SID) 2008 were used to select optimal parameters where differences existed, with a goal to maximize model performance and face validity. Inclusion criteria were not changed and included all discharges for patients <18 years with International Classification of Diseases, Ninth Revision, Clinical Modification procedure codes for congenital heart surgery or nonspecific heart surgery combined with congenital heart disease diagnosis codes. The final model includes procedure risk group, age (0-28 days, 29-90 days, 91-364 days, 1-17 years), low birth weight (500-2499 g), other congenital anomalies (Clinical Classifications Software 217, except for 758.xx), multiple procedures, and transfer-in status. Among 17 945 eligible cases in the SID 2008, the c statistic for model performance was 0.82. In the SID 2013 validation data set, the c statistic was 0.82. Risk-adjusted mortality rates by center ranged from 0.9% to 4.1% (5th-95th percentile).
Congenital heart surgery programs can now obtain national benchmarking reports by applying AHRQ Quality Indicator software to hospital administrative data, based on the harmonized RACHS-1 method, with high discrimination and face validity.
美国国家质量论坛先前批准了一项由医疗保健研究与质量局(AHRQ)制定的先天性心脏手术死亡率质量指标。该指标纳入了经过验证的先天性心脏手术风险调整(RACHS-1)方法的几个参数,但其他参数有所不同。作为美国国家质量论坛认可维护流程的一部分,开发者被要求协调这两种方法。
保留了两种方法中相同的参数。利用AHRQ的医疗成本与利用项目州住院数据库(SID)2008来选择存在差异的最优参数,目标是使模型性能和表面效度最大化。纳入标准未改变,包括所有年龄<18岁患者的出院记录,这些记录具有《国际疾病分类,第九版,临床修订本》先天性心脏手术的程序编码或非特异性心脏手术合并先天性心脏病诊断编码。最终模型包括手术风险组、年龄(0 - 28天、29 - 90天、91 - 364天、1 - 17岁)、低出生体重(500 - 2499克)、其他先天性异常(临床分类软件217,但758.xx除外)、多次手术以及转入状态。在SID 2008的17945例符合条件的病例中,模型性能的c统计量为0.82。在SID 2013验证数据集中,c统计量为0.82。各中心经风险调整的死亡率范围为0.9%至4.1%(第5至95百分位数)。
基于协调后的RACHS-1方法,先天性心脏手术项目现在可以通过将AHRQ质量指标软件应用于医院管理数据来获取全国基准报告,该方法具有较高的区分度和表面效度。