Sulz Michael C, Kröger Arne, Prakash Meher, Manser Christine N, Heinrich Henriette, Misselwitz Benjamin
Division of Gastroenterology and Hepatology, University Hospital Zurich, Zurich, Switzerland.
Division of Gastroenterology and Hepatology, Kantonsspital St. Gallen, St. Gallen, Switzerland.
PLoS One. 2016 Jun 3;11(6):e0154149. doi: 10.1371/journal.pone.0154149. eCollection 2016.
Low-quality bowel preparation reduces efficacy of colonoscopy. We aimed to summarize effects of bowel preparation on detection of adenomas, advanced adenomas and colorectal cancer.
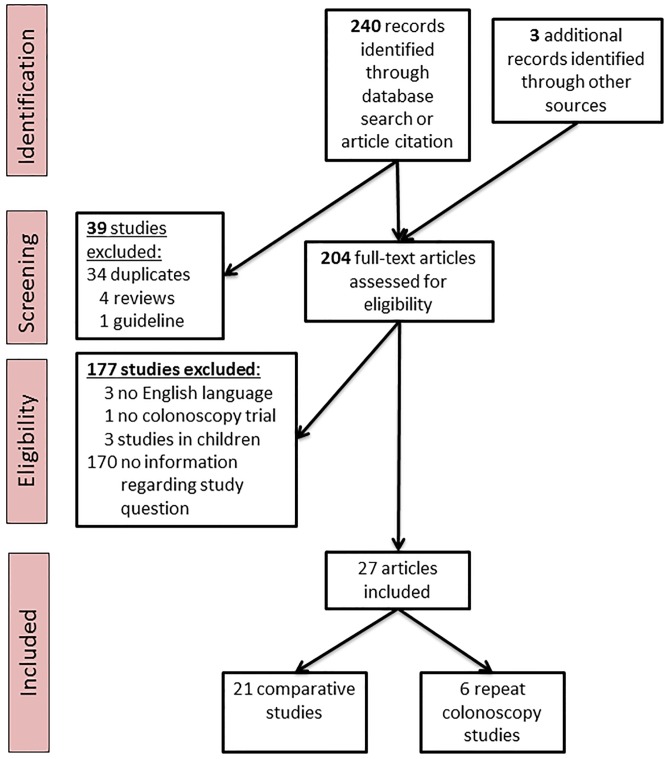
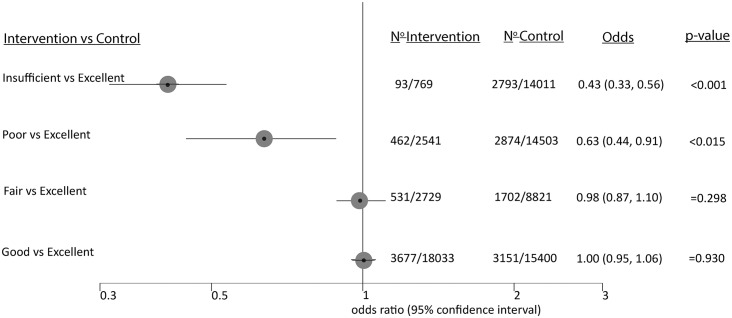
A systematic literature search was performed regarding detection of colonic lesions after normal and low-quality bowel preparation. Reported bowel preparation quality was transformed to the Aronchick scale with its qualities "excellent", "good", "fair", "poor", and "insufficient" or "optimal" (good/excellent), "suboptimal" (fair/poor/insufficient), "adequate" (good/excellent/fair) and "inadequate" (poor/insufficient). We identified two types of studies: i) Comparative studies, directly comparing lesion detection according to bowel preparation quality, and ii) repeat colonoscopy studies, reporting results of a second colonoscopy after previous low-quality preparation.
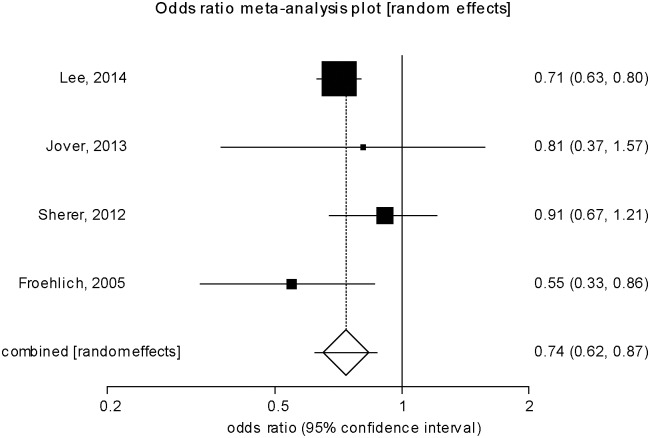
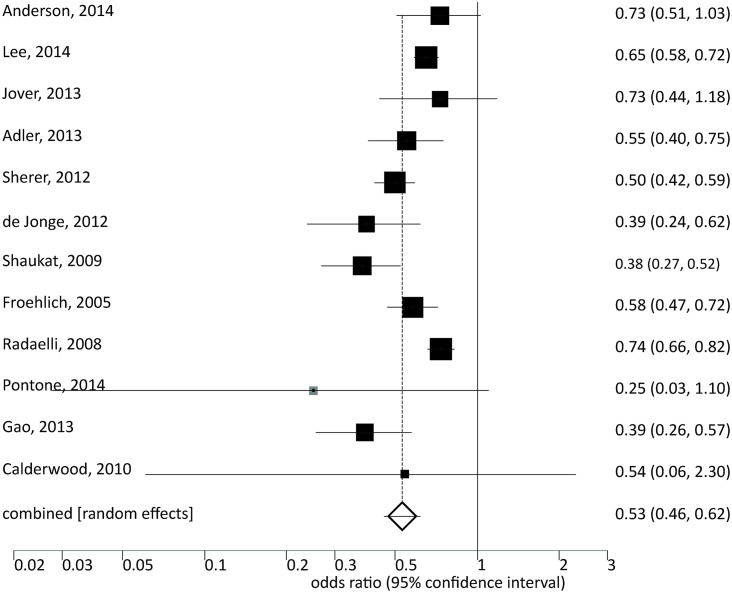
The detection of early adenomas was reduced with inadequate vs. adequate bowel preparation (Odds Ratio (OR) 0.53, CI: 0.46-0.62, p<0.001). The advanced adenomas were affected less in comparison (0.74, CI: 0.62-0.87, p<0.001). The large number of subjects considered in the present meta-analysis resulted in smaller confidence intervals compared to earlier studies. Classifying the bowel-preparation quality as suboptimal vs. optimal led to the same qualitative conclusion (OR: 0.81, CI: 0.74-0.89, p<0.001 for early adenomas, OR: 0.94, CI: 0.87-1.01, n.s. for advanced adenomas). Bowel preparation was equally important for right-sided/ flat/ serrated vs. other lesions in most observational studies but more relevant in some repeat colonoscopy studies; data regarding carcinoma detection were insufficient.
Inadequate bowel preparation affects detection of early colonic lesions stronger than advanced lesions.
低质量的肠道准备会降低结肠镜检查的效果。我们旨在总结肠道准备对腺瘤、高级别腺瘤和结直肠癌检测的影响。
针对正常和低质量肠道准备后结肠病变的检测进行了系统的文献检索。报告的肠道准备质量被转换为阿龙奇克量表,其质量等级为“优秀”“良好”“中等”“差”和“不足”,或“最佳”(良好/优秀)、“次优”(中等/差/不足)、“充分”(良好/优秀/中等)和“不充分”(差/不足)。我们确定了两种类型的研究:i)比较研究,直接根据肠道准备质量比较病变检测情况;ii)重复结肠镜检查研究,报告先前低质量准备后第二次结肠镜检查的结果。
与充分的肠道准备相比,不充分的肠道准备会降低早期腺瘤的检测率(优势比(OR)0.53,置信区间:0.46 - 0.62,p < 0.001)。相比之下,高级别腺瘤受到的影响较小(0.74,置信区间:0.62 - 0.87,p < 0.001)。与早期研究相比,本荟萃分析中纳入的大量受试者导致置信区间更小。将肠道准备质量分类为次优与最佳得出了相同的定性结论(早期腺瘤的OR:0.81,置信区间:0.74 - 0.89,p < 0.001;高级别腺瘤的OR:0.94,置信区间:0.87 - 1.01,无统计学意义)。在大多数观察性研究中,肠道准备对右侧/扁平/锯齿状病变与其他病变同样重要,但在一些重复结肠镜检查研究中更相关;关于癌症检测的数据不足。
不充分的肠道准备对早期结肠病变检测的影响比对高级别病变的影响更大。