Chen Wen-Cheng, Lai Chia-Hsuan, Fang Chiung-Cheng, Yang Yao-Hsu, Chen Pau-Chung, Lee Chuan-Pin, Chen Miao-Fen
From the Department of Radiation Oncology (WCC, CHL, CCF, MFC),Chang Gung Memorial Hospital, Chiayi; College of Medicine (WCC, MFC), Chang Gung University, Taoyuan; Center of Excellence for Chang Gung Research Datalink (WCC, CHL, YHY, PCC, CPL, MFC); Traditional Chinese Medicine (YHY), Chang Gung Memorial Hospital, Chiayi; Institute of Occupational Medicine and Industrial Hygiene (YHY, PCC), National Taiwan University College of Public Health; and Department of Environmental and Occupational Medicine (YHY, PCC), National Taiwan University Hospital and National Taiwan University College of Medicine (PCC), Taipei, Taiwan.
Medicine (Baltimore). 2016 May;95(22):e3770. doi: 10.1097/MD.0000000000003770.
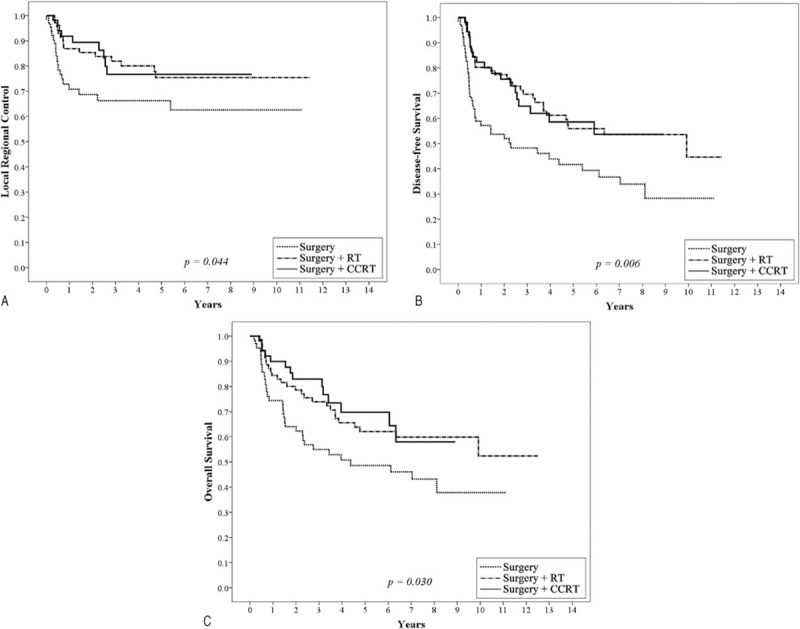
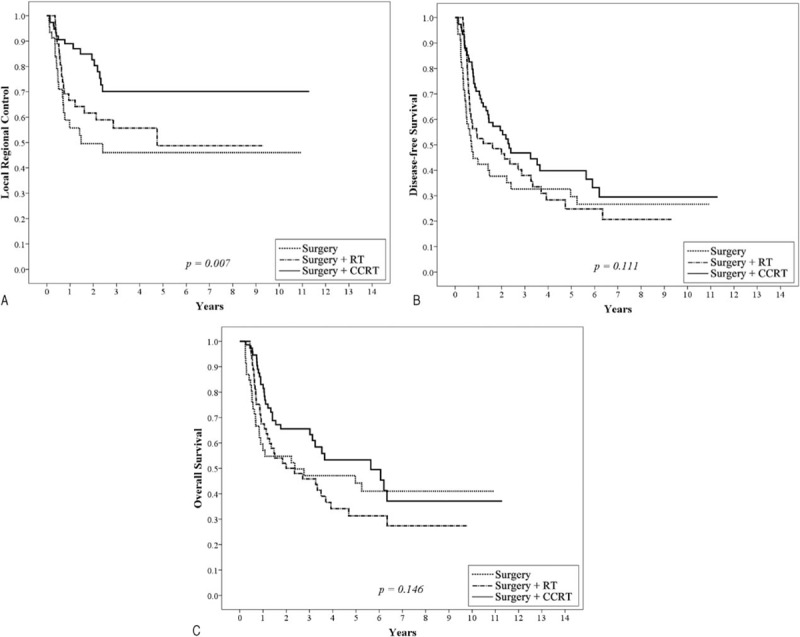
Patients with oral cavity squamous cell carcinoma (OSCC) undergoing surgery are recommended to receive adjuvant radiation therapy with or without chemotherapy if there are unfavorable prognostic factors. A positive resection margin (PRM) and extra-capsular extension (ECE) of lymph nodes are well-known major prognostic factors. However, there is no agreement on whether oral cavity cancer patients should receive postoperative chemo-radiotherapy (CCRT) if they present with other risk factors or a combination of 2 or more risk factors. In this study, we investigated this issue and provide suggestions for adjuvant treatments.From January 2002 to December 2013, 567 OSCC patients who had undergone radical surgery were retrospectively reviewed. The 5-year loco-regional control (LRC), distant metastasis-free (DMF), disease-free survival (DFS), and overall survival (OS) were analyzed.In univariate analysis, pathological T classification, positive node, tumor depth, ECE, lymphatic or vascular or perineural invasion and histology grade are significant prognostic factors for LRC, DMF, DFS, or OS. By multivariate analysis, pathological T4 (pT4), positive node, positive surgical margin are prognostic factors for LRC. pT4, positive node and lymphatic invasion predicted for higher rate of distant metastasis. pT4, positive node, and poor differentiation tumor were prognostic factors for DFS. pT4, positive nodes, and ECE were prognostic factors for OS. These factors were used to define risk groups. We proposed PRM and ECE as major risk factors and pT4, positive nodes, close margin (≤ 5 mm, > 1 mm), tumor depth ≥ 1 cm, lymphatic invasion, vascular invasion, perineural invasion, and poor differentiation as minor risk factors. By subgroups analysis, 192 patients with at least 2 minor prognostic factors and no other major risk factors, postoperative radiotherapy (RT), or CCRT yielded significantly better 5-year LRC, DFS, and OS compared to surgery only group. For 179 patients with at least 3 minor prognostic factors and/or at least 1 major risk factor, patients receiving postoperative CCRT showed significantly better 5-year LRC, DFS, and OS compared with post-OP RT or surgery alone.Patients with 2 minor risk factors should receive postoperative RT. For patients with PRM, ECE, or >2 minor risk factors, postoperative CCRT is recommended.
对于接受手术治疗的口腔鳞状细胞癌(OSCC)患者,如果存在不良预后因素,建议接受辅助放疗,可联合或不联合化疗。切缘阳性(PRM)和淋巴结包膜外扩展(ECE)是众所周知的主要预后因素。然而,对于口腔癌患者如果存在其他危险因素或两种或更多危险因素的组合时是否应接受术后放化疗(CCRT),目前尚无定论。在本研究中,我们对这一问题进行了调查,并为辅助治疗提供建议。
回顾性分析了2002年1月至2013年12月期间567例行根治性手术的OSCC患者。分析了5年局部区域控制率(LRC)、无远处转移率(DMF)、无病生存率(DFS)和总生存率(OS)。
单因素分析中,病理T分期、阳性淋巴结、肿瘤深度、ECE、淋巴管或血管或神经周围侵犯以及组织学分级是LRC、DMF、DFS或OS的显著预后因素。多因素分析显示,病理T4(pT4)、阳性淋巴结、手术切缘阳性是LRC的预后因素。pT4、阳性淋巴结和淋巴管侵犯预示着更高的远处转移率。pT4、阳性淋巴结和低分化肿瘤是DFS的预后因素。pT4、阳性淋巴结和ECE是OS的预后因素。这些因素用于定义风险组。我们提出PRM和ECE为主要危险因素,pT4、阳性淋巴结、切缘接近(≤5mm,>1mm)、肿瘤深度≥1cm、淋巴管侵犯、血管侵犯、神经周围侵犯和低分化为次要危险因素。亚组分析显示,192例至少有2个次要预后因素且无其他主要危险因素的患者,与单纯手术组相比,术后放疗(RT)或CCRT的5年LRC、DFS和OS显著更好。对于179例至少有3个次要预后因素和/或至少1个主要危险因素的患者,接受术后CCRT的患者与术后RT或单纯手术相比,5年LRC、DFS和OS显著更好。
有2个次要危险因素的患者应接受术后RT。对于有PRM、ECE或>2个次要危险因素的患者,建议术后CCRT。