Kenya Medical Research Institute (KEMRI)/Wellcome Trust Research Programme, Kilifi, Kenya; Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK.
Kenya Medical Research Institute (KEMRI)/Wellcome Trust Research Programme, Kilifi, Kenya.
Lancet Glob Health. 2016 Jul;4(7):e464-73. doi: 10.1016/S2214-109X(16)30096-1. Epub 2016 Jun 2.
Children with complicated severe acute malnutrition (SAM) have a greatly increased risk of mortality from infections while in hospital and after discharge. In HIV-infected children, mortality and admission to hospital are prevented by daily co-trimoxazole prophylaxis, despite locally reported bacterial resistance to co-trimoxazole. We aimed to assess the efficacy of daily co-trimoxazole prophylaxis on survival in children without HIV being treated for complicated SAM.
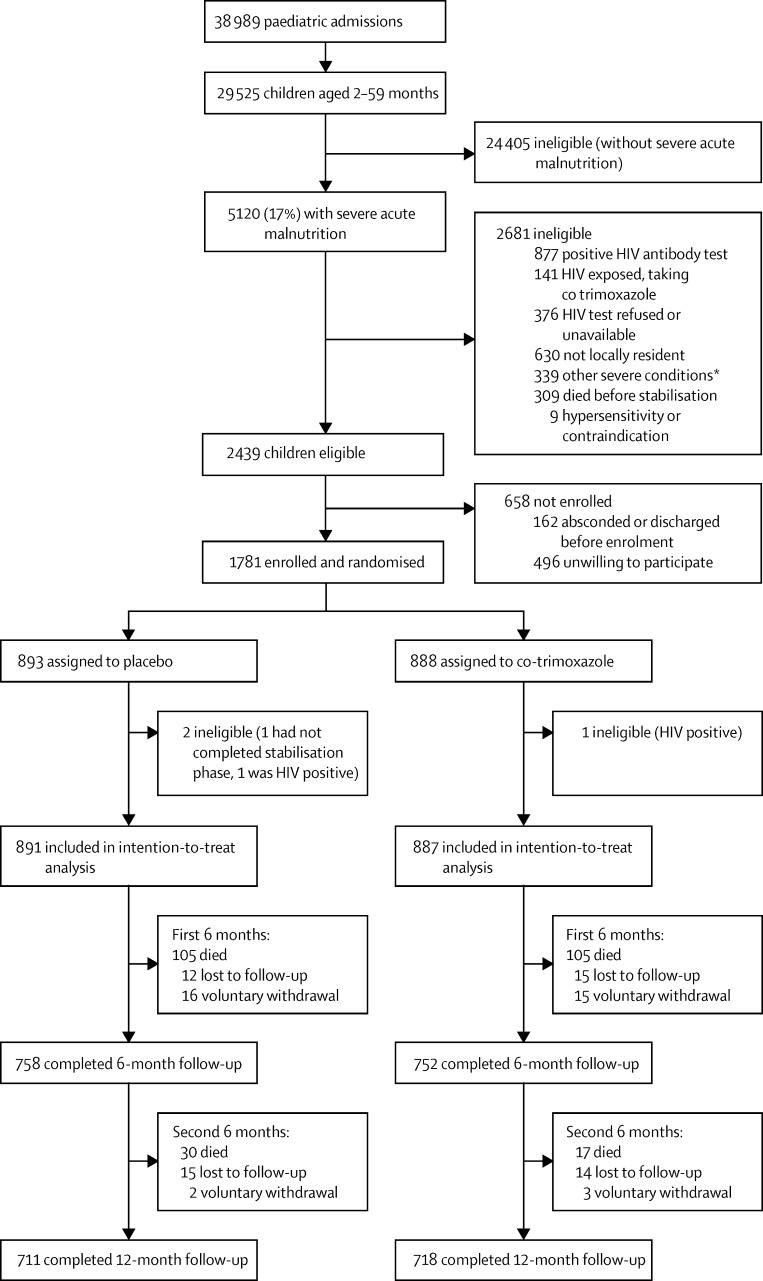
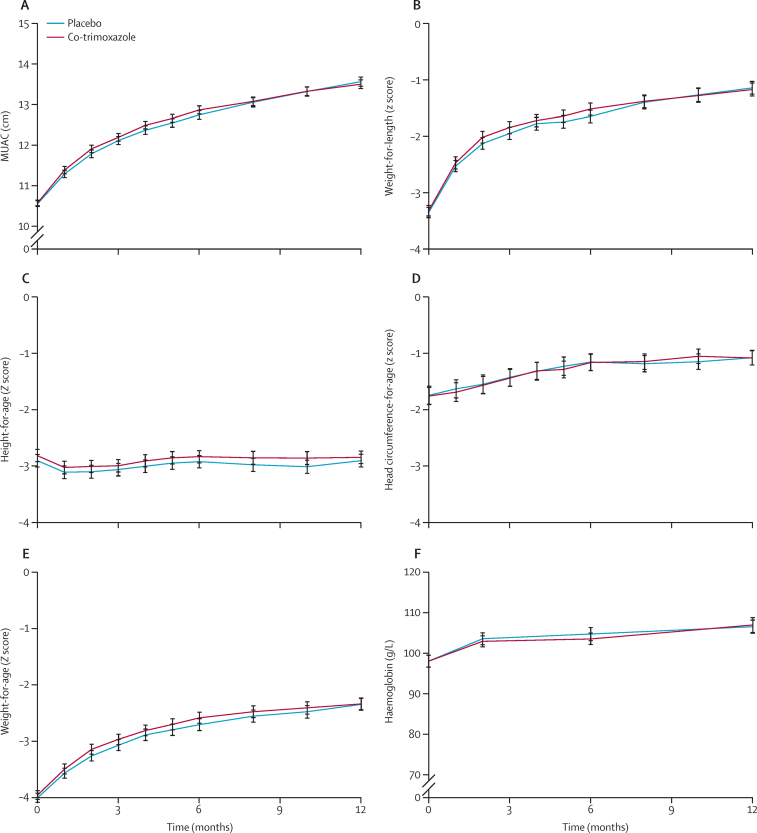
We did a multicentre, double-blind, randomised, placebo-controlled study in four hospitals in Kenya (two rural hospitals in Kilifi and Malindi, and two urban hospitals in Mombasa and Nairobi) with children aged 60 days to 59 months without HIV admitted to hospital and diagnosed with SAM. We randomly assigned eligible participants (1:1) to 6 months of either daily oral co-trimoxazole prophylaxis (given as water-dispersible tablets; 120 mg per day for age <6 months, 240 mg per day for age 6 months to 5 years) or matching placebo. Assignment was done with computer-generated randomisation in permuted blocks of 20, stratified by centre and age younger or older than 6 months. Treatment allocation was concealed in opaque, sealed envelopes and patients, their families, and all trial staff were masked to treatment assignment. Children were given recommended medical care and feeding, and followed up for 12 months. The primary endpoint was mortality, assessed each month for the first 6 months, then every 2 months for the second 6 months. Secondary endpoints were nutritional recovery, readmission to hospital, and illness episodes treated as an outpatient. Analysis was by intention to treat. This trial was registered at ClinicalTrials.gov, number NCT00934492.
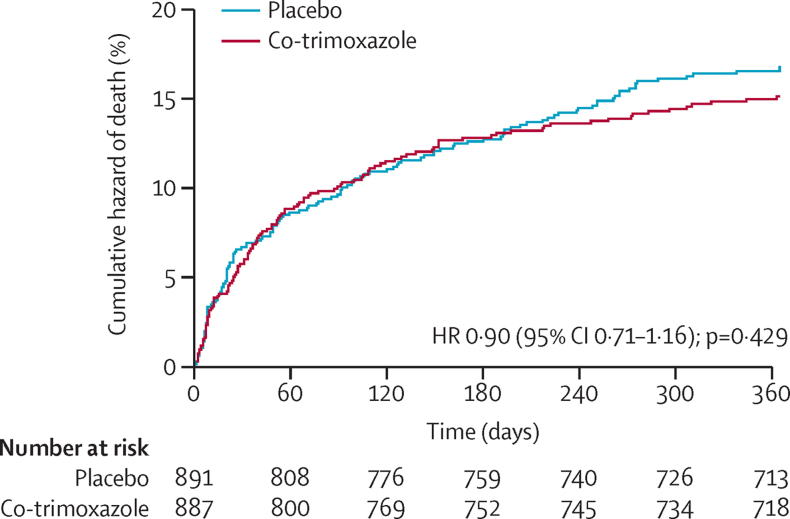
Between Nov 20, 2009, and March 14, 2013, we recruited and assigned 1778 eligible children to treatment (887 to co-trimoxazole prophylaxis and 891 to placebo). Median age was 11 months (IQR 7-16 months), 306 (17%) were younger than 6 months, 300 (17%) had oedematous malnutrition (kwashiorkor), and 1221 (69%) were stunted (length-for-age Z score <-2). During 1527 child-years of observation, 122 (14%) of 887 children in the co-trimoxazole group died, compared with 135 (15%) of 891 in the placebo group (unadjusted hazard ratio [HR] 0·90, 95% CI 0·71-1·16, p=0·429; 16·0 vs 17·7 events per 100 child-years observed (CYO); difference -1·7 events per 100 CYO, 95% CI -5·8 to 2·4]). In the first 6 months of the study (while participants received study medication), 63 suspected grade 3 or 4 associated adverse events were recorded among 57 (3%) children; 31 (2%) in the co-trimoxazole group and 32 (2%) in the placebo group (incidence rate ratio 0·98, 95% CI 0·58-1·65). The most common adverse events of these grades were urticarial rash (grade 3, equally common in both groups), neutropenia (grade 4, more common in the co-trimoxazole group), and anaemia (both grades equally common in both groups). One child in the placebo group had fatal toxic epidermal necrolysis with concurrent Pseudomonas aeruginosa bacteraemia.
Daily co-trimoxazole prophylaxis did not reduce mortality in children with complicated SAM without HIV. Other strategies need to be tested in clinical trials to reduce deaths in this population.
Wellcome Trust, UK.
患有复杂严重急性营养不良(SAM)的儿童在住院期间和出院后因感染而死亡的风险大大增加。在感染 HIV 的儿童中,尽管局部报告了对复方磺胺甲噁唑的细菌耐药性,但每日联合磺胺甲噁唑预防可预防死亡率和住院率。我们旨在评估在没有 HIV 的接受复杂严重急性营养不良(SAM)治疗的儿童中,每日联合磺胺甲噁唑预防对生存的疗效。
我们在肯尼亚的四家医院(基利菲和马林迪的两家农村医院,以及蒙巴萨和内罗毕的两家城市医院)进行了一项多中心、双盲、随机、安慰剂对照研究,纳入年龄在 60 天至 59 个月、无 HIV 且诊断为 SAM 的住院儿童。我们将符合条件的参与者(1:1)随机分配接受 6 个月的每日口服复方磺胺甲噁唑预防(给予可分散的片剂;年龄<6 个月的每天 120mg,年龄 6 个月至 5 岁的每天 240mg)或匹配的安慰剂。采用计算机生成的随机化方法,以 20 个为一组的置换块进行分组,按中心和年龄(<6 个月或≥6 个月)分层。治疗分配采用不透明、密封的信封进行隐藏,患者、他们的家人和所有试验工作人员对治疗分配均进行盲法处理。患儿接受推荐的医疗和喂养,并随访 12 个月。主要终点是死亡率,在前 6 个月每月评估一次,然后在第 2 个 6 个月每 2 个月评估一次。次要终点是营养恢复、再次住院和门诊治疗的疾病发作。分析采用意向治疗。该试验在 ClinicalTrials.gov 注册,编号为 NCT00934492。
在 2009 年 11 月 20 日至 2013 年 3 月 14 日期间,我们招募并分配了 1778 名符合条件的患儿进行治疗(887 名接受复方磺胺甲噁唑预防,891 名接受安慰剂)。中位年龄为 11 个月(IQR 7-16 个月),306 名(17%)年龄<6 个月,300 名(17%)有水肿性营养不良(夸希奥科),1221 名(69%)身材矮小(年龄-身高 Z 评分<-2)。在 1527 个儿童年观察期间,887 名接受复方磺胺甲噁唑预防的患儿中有 122 名(14%)死亡,而 891 名接受安慰剂的患儿中有 135 名(15%)(未调整的危险比[HR]0·90,95%CI 0·71-1·16,p=0·429;16·0 与 17·7 例每 100 个儿童年观察(CYO)的事件;差异-1·7 例 CYO,95%CI-5·8 至 2·4))。在研究的前 6 个月(在参与者接受研究药物期间),57 名(3%)患儿中记录了 63 例疑似 3 级或 4 级相关不良事件;31 名(2%)在复方磺胺甲噁唑预防组,32 名(2%)在安慰剂组(发病率比 0·98,95%CI 0·58-1·65)。这些严重程度的最常见不良事件是荨麻疹(3 级,两组发生率相同)、中性粒细胞减少症(4 级,复方磺胺甲噁唑预防组更常见)和贫血(两组发生率相同)。安慰剂组的一名患儿发生了致命的中毒性表皮坏死松解症,伴有铜绿假单胞菌败血症。
在没有 HIV 的患有复杂严重急性营养不良(SAM)的儿童中,每日联合磺胺甲噁唑预防并不能降低死亡率。需要在临床试验中测试其他策略,以减少这一人群的死亡。
英国惠康信托基金会。