Tsurukiri Junya, Ohta Shoichi, Mishima Shiro, Homma Hiroshi, Okumura Eitaro, Akamine Itsuro, Ueno Masahito, Oda Jun, Yukioka Tetsuo
From the Emergency and Critical Care Medicine (J.T., E.O., I.A.), Tokyo Medical University Hachioji Medical Center; Emergency and Disaster Medicine (S.O., S.M., H.H., J.O., T.Y.), Tokyo Medical University, Tokyo, Japan; and General Surgery (M.U.), Fuchinobe General Hospital, Kanagawa, Japan.
J Trauma Acute Care Surg. 2017 Jan;82(1):126-132. doi: 10.1097/TA.0000000000001154.
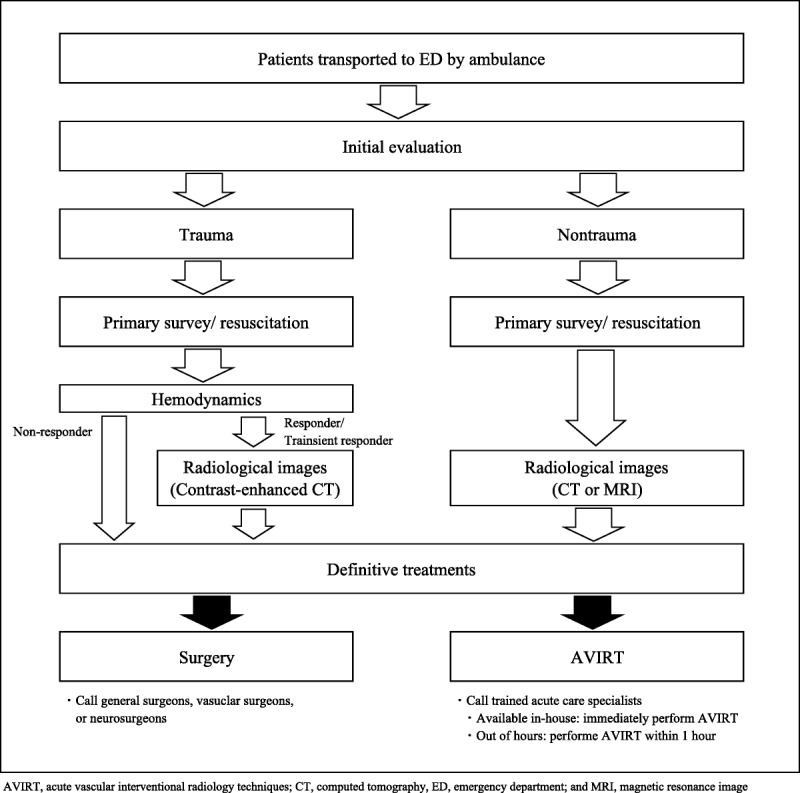
Comprehensive treatment of a patient in acute medicine and surgery requires the use of both surgical techniques and other treatment methods. Recently, acute vascular interventional radiology techniques (AVIRTs) have become increasingly popular, enabling adequately trained in-house experts to improve the quality of on-site care.
After obtaining approval from our institutional ethics committee, we conducted a retrospective study of AVIRT procedures performed by acute care specialists trained in acute medicine and surgery over a 1-year period, including those conducted out of hours. Trained acute care specialists were required to be certified by the Japanese Association of Acute Medicine and to have completed at least 1 year of training as a member of the endovascular team in the radiology department of another university hospital. The study was designed to ensure that at least one of the physicians was available to perform AVIRT within 1 h of a request at any time. Femoral sheath insertion was usually performed by the resident physicians under the guidance of trained acute care specialists.
The study sample comprised 77 endovascular procedures for therapeutic AVIRT (trauma, n = 29, and nontrauma, n = 48) among 62 patients (mean age, 64 years; range, 9-88 years), of which 55% were male. Of the procedures, 47% were performed out of hours (trauma, 52%; and nontrauma, 44%). Three patients underwent resuscitative endovascular balloon occlusion of the aorta in the emergency room. No major device-related complications were encountered, and the overall mortality rate within 60 days was 8%. The recorded causes of death included exsanguination (n = 2), pneumonia (n = 2), sepsis (n = 1), and brain death (n = 1).
When performed by trained acute care specialists, AVIRT seems to be advantageous for acute on-site care and provides good technical success. Therefore, a standard training program should be established for acute care specialists or trauma surgeons to make these techniques a part of the standard regimen.
Therapy/care management study, level V.
对急重症内科和外科患者进行综合治疗需要同时运用外科技术和其他治疗方法。近年来,急性血管介入放射技术(AVIRTs)越来越受欢迎,使训练有素的院内专家能够提高现场护理质量。
在获得我院伦理委员会批准后,我们对急重症内科和外科训练有素的急性护理专家在1年期间进行的AVIRT手术进行了回顾性研究,包括非工作时间进行的手术。训练有素的急性护理专家须获得日本急性医学协会认证,并在另一所大学医院放射科作为血管内治疗团队成员完成至少1年的培训。该研究旨在确保随时有至少一名医生能够在接到请求后1小时内进行AVIRT手术。股动脉鞘置入通常由住院医师在训练有素的急性护理专家指导下进行。
研究样本包括62例患者(平均年龄64岁;范围9 - 88岁)中的77例治疗性AVIRT血管内手术(创伤29例,非创伤48例),其中55%为男性。这些手术中,47%在非工作时间进行(创伤52%,非创伤44%)。3例患者在急诊室接受了复苏性主动脉内球囊阻断术。未出现与器械相关的重大并发症,60天内总死亡率为8%。记录的死亡原因包括失血(2例)、肺炎(2例)、败血症(1例)和脑死亡(1例)。
由训练有素的急性护理专家进行AVIRT手术,似乎对急性现场护理有利,并能取得良好的技术成功率。因此,应为急性护理专家或创伤外科医生制定标准培训计划,使这些技术成为标准治疗方案的一部分。
治疗/护理管理研究,V级。