Kaushal Mohinder
Arthroscopy and Spinal Endoscopy Centre, Chandigarh, India; Department of Orthopedics, Trinity Hospital and Medical Research Institute, Chandigarh, India.
Indian J Orthop. 2016 May-Jun;50(3):228-33. doi: 10.4103/0019-5413.181777.
Avaialable minimal invasive arthro/endoscopic techniques are not compatible with 30 degree arthroscope which orthopedic surgeons uses in knee and shoulder arthroscopy. Minimally invasive "Arthrospine assisted percutaneous technique for lumbar discectomy" is an attempt to allow standard familiar microsurgical discectomy and decompression to be performed using 30° arthroscope used in knee and shoulder arthroscopy with conventional micro discectomy instruments.
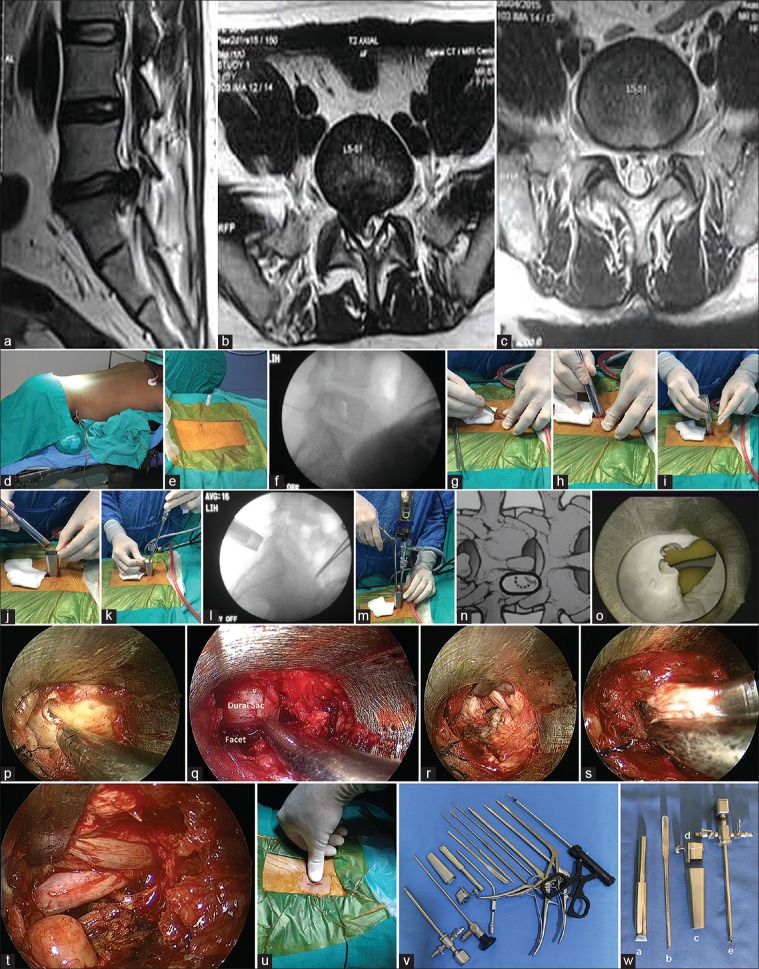
150 patients suffering from lumbar disc herniations were operated between January 2004 and December 2012 by indiginously designed Arthrospine system and were evaluated retrospectively. In lumbar discectomy group, there were 85 males and 65 females aged between 18 and 72 years (mean, 38.4 years). The delay between onset of symptoms to surgery was between 3 months to 7 years. Levels operated upon included L1-L2 (n = 3), L2-L3 (n = 2), L3-L4 (n = 8), L4-L5 (n = 90), and L5-S1 (n = 47). Ninety patients had radiculopathy on right side and 60 on left side. There were 22 central, 88 paracentral, 12 contained, 3 extraforaminal, and 25 sequestrated herniations. Standard protocol of preoperative blood tests, x-ray LS Spine and pre operative MRI and pre anaesthetic evaluation for anaesthesia was done in all cases. Technique comprised localization of symptomatic level followed by percutaneous dilatation and insertion of a newly devised arthrospine system devise over a dilator through a 15 mm skin and fascial incision. Arthro/endoscopic discectomy was then carried out by 30° arthroscope and conventional disc surgery instruments.
Based on modified Macnab's criteria, of 150 patients operated for lumbar discectomy, 136 (90%) patients had excellent to good, 12 (8%) had fair, and 2 patients (1.3%) had poor results. The complications observed were discitis in 3 patients (2%), dural tear in 4 patients (2.6%), and nerve root injury in 2 patients (1.3%). About 90% patients were able to return to light and sedentary work with an average delay of 2 weeks and normal physical activities after 2 months.
Arthrospine system is compatible with 30° arthroscope and conventional micro-discectomy instruments. Technique minimizes approach related morbidity and provides minimal access corridor for lumbar discectomy.
现有的微创关节镜/内窥镜技术与骨科医生在膝关节和肩关节镜检查中使用的30度关节镜不兼容。微创“关节镜辅助经皮腰椎间盘切除术技术”试图使用膝关节和肩关节镜检查中使用的30°关节镜以及传统的显微椎间盘切除术器械来进行标准的熟悉的显微外科椎间盘切除术和减压术。
2004年1月至2012年12月期间,对150例腰椎间盘突出症患者采用自行设计的关节镜系统进行手术,并进行回顾性评估。在腰椎间盘切除术组中,男性85例,女性65例,年龄在18至72岁之间(平均38.4岁)。症状出现至手术的延迟时间为3个月至7年。手术节段包括L1-L2(n = 3)、L2-L3(n = 2)、L3-L4(n = 8)、L4-L5(n = 90)和L5-S1(n = 47)。90例患者右侧有神经根病,60例左侧有神经根病。有22例中央型、88例旁中央型、12例包容性、3例椎间孔外型和25例游离型椎间盘突出。所有病例均进行了术前血液检查、腰骶部脊柱X线检查、术前MRI检查以及麻醉前麻醉评估的标准方案。技术包括确定有症状的节段,然后经皮扩张,并通过一个15毫米的皮肤和筋膜切口在扩张器上插入一个新设计的关节镜系统装置。然后用30°关节镜和传统的椎间盘手术器械进行关节镜/内窥镜下椎间盘切除术。
根据改良的Macnab标准,在150例行腰椎间盘切除术的患者中,136例(90%)患者效果为优至良,12例(8%)效果为一般,2例(1.3%)效果差。观察到的并发症包括3例(2%)椎间盘炎、4例(2.6%)硬脊膜撕裂和2例(1.3%)神经根损伤。约90%的患者能够恢复轻度和久坐的工作,平均延迟2周,2个月后恢复正常体力活动。
关节镜系统与30°关节镜和传统的显微椎间盘切除术器械兼容。该技术将手术入路相关的发病率降至最低,并为腰椎间盘切除术提供了最小的手术通道。