Matthews Anthony, Langan Sinéad M, Douglas Ian J, Smeeth Liam, Bhaskaran Krishnan
Department of Non-Communicable Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, United Kingdom.
PLoS Med. 2016 Jun 14;13(6):e1002037. doi: 10.1371/journal.pmed.1002037. eCollection 2016 Jun.
Laboratory evidence suggests that reduced phosphodiesterase type 5 (PDE5) expression increases the invasiveness of melanoma cells; hence, pharmacological inhibition of PDE5 could affect melanoma risk. Two major epidemiological studies have investigated this and come to differing conclusions. We therefore aimed to investigate whether PDE5 inhibitor use is associated with an increased risk of malignant melanoma, and whether any increase in risk is likely to represent a causal relationship.
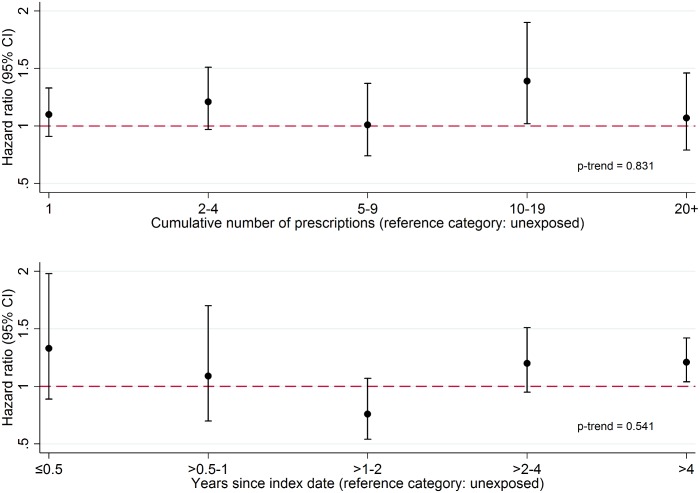
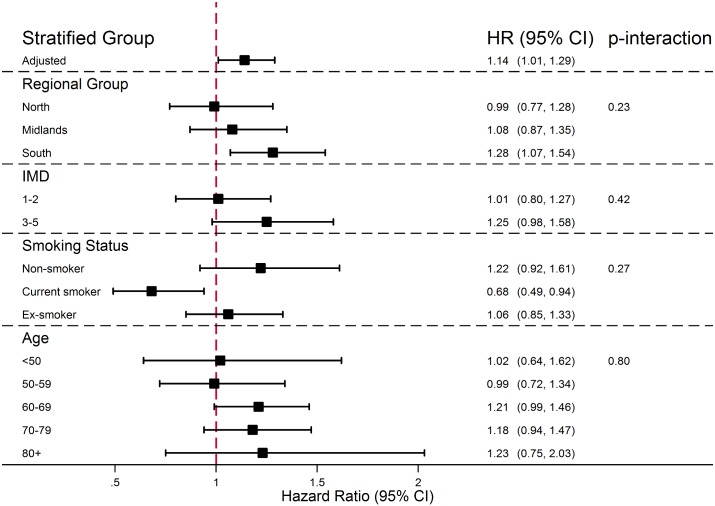
We conducted a matched cohort study using primary care data from the UK Clinical Practice Research Datalink. All men initiating a PDE5 inhibitor and with no prior cancer diagnosis were identified and matched on age, diabetes status, and general practice to up to four unexposed controls. Ever use of a PDE5 inhibitor and time-updated cumulative number of PDE5 inhibitor prescriptions were investigated as exposures, and the primary outcome was malignant melanoma. Basal cell carcinoma, solar keratosis, and colorectal cancer were investigated as negative control outcomes to exclude bias. Hazard ratios (HRs) were estimated from Cox models stratified by matched set and adjusted for potential confounders. 145,104 men with ≥1 PDE5 inhibitor prescription, and 560,933 unexposed matched controls were included. In total, 1,315 incident malignant melanoma diagnoses were observed during 3.44 million person-years of follow-up (mean 4.9 y per person). After adjusting for potential confounders, there was weak evidence of a small positive association between PDE5 inhibitor use and melanoma risk (HR = 1.14, 95% CI 1.01-1.29, p = 0.04). A similar increase in risk was seen for the two negative control outcomes related to sun exposure (HR = 1.15, 95% CI 1.11-1.19, p < 0.001, for basal cell carcinoma; HR = 1.21, 95% CI 1.17-1.25, p < 0.001, for solar keratosis), but there was no increased risk for colorectal cancer (HR = 0.91, 95% CI 0.85-0.98, p = 0.01). There was no evidence that risk increased with number of prescriptions received (p-trend = 0.83). In a post hoc analysis, there was strong evidence that solar keratosis was associated with future PDE5 inhibitor use (odds ratio = 1.28, 95% CI 1.23-1.34, p < 0.001), suggesting that men with higher sun exposure were more likely to become PDE5 inhibitor users. However, a limitation of our study was that we did not have individual-level data on sun exposure, so we could not directly control for this in the primary analysis.
Our results were not consistent with PDE5 inhibitors being causally associated with melanoma risk, and strongly suggest that observed risk increases are driven by greater sun exposure among patients exposed to a PDE5 inhibitor.
实验室证据表明,5型磷酸二酯酶(PDE5)表达降低会增加黑色素瘤细胞的侵袭性;因此,PDE5的药理学抑制可能会影响黑色素瘤风险。两项主要的流行病学研究对此进行了调查,但得出了不同的结论。因此,我们旨在研究使用PDE5抑制剂是否与恶性黑色素瘤风险增加相关,以及风险的任何增加是否可能代表因果关系。
我们利用英国临床实践研究数据链中的初级保健数据进行了一项匹配队列研究。识别出所有开始使用PDE5抑制剂且既往无癌症诊断的男性,并根据年龄、糖尿病状态和全科医疗情况与多达4名未暴露的对照进行匹配。将曾经使用PDE5抑制剂以及PDE5抑制剂处方的时间更新累积数量作为暴露因素进行研究,主要结局为恶性黑色素瘤。将基底细胞癌、日光性角化病和结直肠癌作为阴性对照结局进行研究,以排除偏倚。通过按匹配组分层并针对潜在混杂因素进行调整的Cox模型估计风险比(HR)。纳入了145,104名有≥1次PDE5抑制剂处方的男性以及560,933名未暴露的匹配对照。在344万人年的随访期间(平均每人4.9年),共观察到1,315例恶性黑色素瘤确诊病例。在调整潜在混杂因素后,有微弱证据表明使用PDE5抑制剂与黑色素瘤风险之间存在小的正相关(HR = 1.14,95% CI 1.01 - 1.29,p = 0.04)。与阳光暴露相关的两个阴性对照结局也出现了类似的风险增加(基底细胞癌的HR = 1.15,95% CI 1.11 - 1.19,p < 0.001;日光性角化病的HR = 1.21,95% CI 1.17 - 1.25,p < 0.001),但结直肠癌风险没有增加(HR = 0.91,95% CI 0.85 - 0.98,p = 0.01)。没有证据表明风险随接受的处方数量增加而增加(p趋势 = 0.83)。在一项事后分析中,有强有力的证据表明日光性角化病与未来使用PDE5抑制剂相关(优势比 = 1.28,95% CI 1.23 - 1.34,p < 0.001),这表明阳光暴露较高的男性更有可能成为PDE5抑制剂使用者。然而,我们研究的一个局限性是我们没有关于阳光暴露的个体水平数据,因此在主要分析中无法直接对此进行控制。
我们的结果与PDE5抑制剂与黑色素瘤风险存在因果关系不一致,强烈表明观察到的风险增加是由暴露于PDE5抑制剂的患者中更高的阳光暴露所驱动。