Goto Tadahiro, Yoshida Kazuki, Tsugawa Yusuke, Filbin Michael R, Camargo Carlos A, Hasegawa Kohei
Department of Emergency Medicine, University of Fukui Hospital, Fukui, Japan.
Department of Emergency Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
BMC Infect Dis. 2016 Jun 14;16:294. doi: 10.1186/s12879-016-1620-1.
We aimed to investigate mortality trends in hospitalized patients with septic shock in the US. To achieve this objective, we tested hypothesis that mortality decreased in patients identified by the code of septic shock while mortality did not change in those with septic shock identified by vasopressor use.
We conducted a serial cross-sectional analysis using Nationwide Inpatient Sample database from 2005 through 2011. First, we identified all adult patients aged ≥18 years hospitalized for septic shock by the following criteria: 1) primary ICD-9 diagnosis of infection plus procedure code for vasopressor use, 2) primary ICD-9 diagnosis of infection plus septic shock in non-primary field, and 3) primary ICD-9 diagnosis of septic shock. Second, we stratified all identified patients by record of vasopressor use. The outcome of interest was year-to-year changes in the in-hospital all-cause mortality.
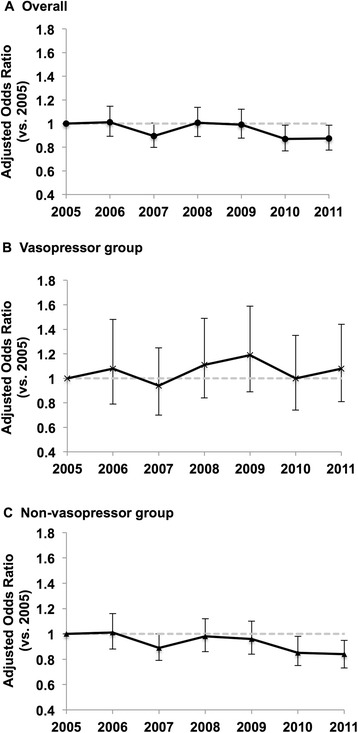
From 2005 to 2011, we identified 109,812 weighted hospitalizations with septic shock. Overall, there was a significant downward trend in in-hospital mortality (from 46 % in 2005 to 42 % in 2011; P trend = 0.003); the adjusted mortality also decreased significantly (OR for comparison of 2005 with 2011, 0.98; 95 % CI, 0.96-1.00; P < 0.001). In stratified analysis, the mortality trend was not significant in the subgroup with vasopressor use (from 42 % in 2005 to 40 % in 2011; P trend =0.57); similarly, the adjusted mortality did not change significantly (OR, 1.01; 95 % CI, 0.97-1.05; P =0.62). By contrast, there was a downward trend in mortality in the subgroup without vasopressor use (from 47 % in 2005 to 43 % in 2011; P trend =0.002); likewise, the adjusted mortality decreased significantly (OR, 0.97; 95 % CI, 0.95-0.99; P =0.002) CONCLUSIONS: From 2005 to 2011, we found a modest decrease in in-hospital mortality among patients identified with septic shock. However, in the subgroup with vasopressor use, we found no significant change in mortality. Our data challenge the conventional wisdom that mortality in this population has improved during the last decade.
我们旨在调查美国感染性休克住院患者的死亡率趋势。为实现这一目标,我们检验了以下假设:通过感染性休克编码识别的患者死亡率下降,而通过血管活性药物使用识别的感染性休克患者死亡率未发生变化。
我们使用2005年至2011年的全国住院患者样本数据库进行了系列横断面分析。首先,我们根据以下标准确定所有年龄≥18岁因感染性休克住院的成年患者:1)原发性ICD - 9感染诊断加血管活性药物使用的操作编码;2)原发性ICD - 9感染诊断加非主要领域的感染性休克;3)原发性ICD - 9感染性休克诊断。其次,我们根据血管活性药物使用记录对所有识别出的患者进行分层。感兴趣的结局是住院全因死亡率的逐年变化。
2005年至2011年,我们识别出109,812例加权的感染性休克住院病例。总体而言,住院死亡率有显著下降趋势(从2005年的46%降至2011年的42%;P趋势=0.003);校正后的死亡率也显著下降(2005年与2011年比较的OR为0.98;95%CI,0.96 - 1.00;P<0.001)。在分层分析中,使用血管活性药物的亚组死亡率趋势不显著(从2005年的42%降至2011年的40%;P趋势=0.57);同样,校正后的死亡率没有显著变化(OR为1.01;95%CI,0.97 - 1.05;P =0.62)。相比之下,未使用血管活性药物的亚组死亡率有下降趋势(从2005年的47%降至2011年的43%;P趋势=0.002);同样,校正后的死亡率显著下降(OR为0.97;95%CI,0.95 - 0.99;P =0.002)。结论:2005年至2011年,我们发现感染性休克患者的住院死亡率有适度下降。然而,在使用血管活性药物的亚组中,我们发现死亡率没有显著变化。我们的数据挑战了过去十年该人群死亡率有所改善的传统观念。