Koganti S, Patel N, Seraphim A, Kotecha T, Whitbread M, Rakhit R D
Department of Cardiology, Royal Free Hospital, London, UK UCL Institute of Cardiovascular Sciences, London, UK.
Department of Cardiology, Royal Free Hospital, London, UK.
BMJ Open. 2016 Jun 20;6(6):e010428. doi: 10.1136/bmjopen-2015-010428.
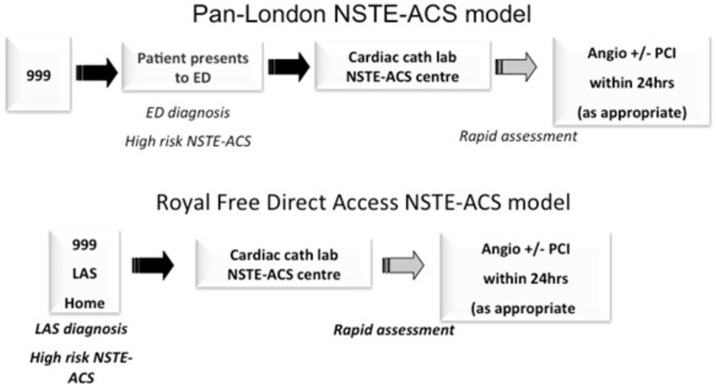
To assess whether a novel 'direct access pathway' (DAP) for the management of high-risk non-ST-elevation acute coronary syndromes (NSTEACS) is safe, results in 'shorter time to intervention and shorter admission times'. This pathway was developed locally to enable London Ambulance Service to rapidly transfer suspected high-risk NSTEACS from the community to our regional heart attack centre for consideration of early angiography.
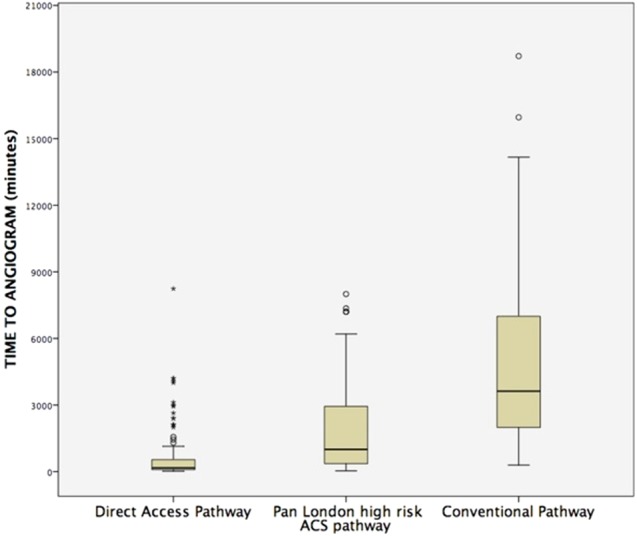
This is a retrospective case-control analysis of 289 patients comparing patients with high-risk NSTEACS admitted via DAP with age-matched controls from the standard pan-London high-risk ACS pathway (PLP) and the conventional pathway (CP). The primary end point of the study was time from admission to coronary angiography/intervention. Secondary end point was total length of hospital stay.
Over a period of 43 months, 101 patients were admitted by DAP, 109 matched patients by PLP and 79 matched patients through CP. Median times from admission to coronary angiography for DAP, PLP and CP were 2.8 (1.5-9), 16.6 (6-50) and 60 (33-116) hours, respectively (p<0.001). Median length of hospital stay for DAP and PLP was similar at 3.0 (2.0-5.0) days in comparison to 5 (3-7) days for CP (p<0.001).
DAP resulted in a significant reduction in time to angiography for patients with high-risk NSTEACS when compared to existing pathways.
评估一种用于管理高危非ST段抬高型急性冠状动脉综合征(NSTEACS)的新型“直接接入途径”(DAP)是否安全,是否能“缩短干预时间和住院时间”。该途径是在本地开发的,旨在使伦敦救护车服务中心能够迅速将疑似高危NSTEACS患者从社区转运至我们的地区心脏病发作中心,以便考虑早期血管造影。
这是一项对289例患者进行的回顾性病例对照分析,将通过DAP入院的高危NSTEACS患者与来自全伦敦标准高危急性冠状动脉综合征途径(PLP)和传统途径(CP)的年龄匹配对照患者进行比较。研究的主要终点是从入院到冠状动脉造影/干预的时间。次要终点是住院总时长。
在43个月的时间里,101例患者通过DAP入院,109例匹配患者通过PLP入院,79例匹配患者通过CP入院。DAP、PLP和CP从入院到冠状动脉造影的中位时间分别为2.8(1.5 - 9)小时、16.6(6 - 50)小时和60(33 - 116)小时(p<0.001)。DAP和PLP的中位住院时长相似,为3.0(2.0 - 5.0)天,而CP为5(3 - 7)天(p<0.001)。
与现有途径相比,DAP显著缩短了高危NSTEACS患者的血管造影时间。