Agyeman Akosua Adom, Ofori-Asenso Richard
Research Unit, Health Policy Consult, Weija, P. O. Box WJ 537, Accra, Ghana.
Ann Clin Microbiol Antimicrob. 2016 Jun 22;15(1):41. doi: 10.1186/s12941-016-0156-y.
Treatment options for drug-resistant tuberculosis are still limited. Linezolid has been recommended for treatment of patients with multidrug-resistant (MDR) or extensively-drug-resistant (XDR) tuberculosis, although uncertainties remain regarding its safety and tolerability in these circumstances.
To systematically evaluate the existing evidence regarding the efficacy and tolerability of linezolid in the treatment of MDR or XDR tuberculosis.
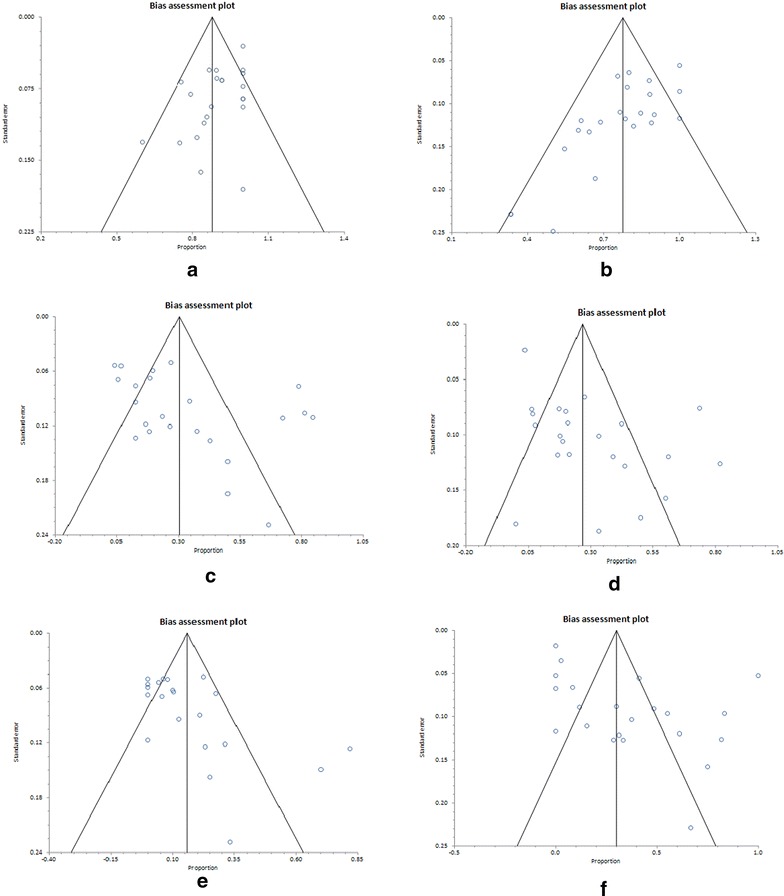
We conducted a systematic review and meta-analysis in accordance with the PRISMA guidelines. Searches were conducted in PubMed, Web of Science and EMBASE followed by direct search of abstracts in the International Journal of Tuberculosis and Lung Disease to retrieve primary studies published between January 2000 and January 2016 assessing linezolid efficacy and safety in the treatment of drug-resistant TB. We evaluated the occurrence of outcomes including culture conversion, treatment success and incidence of adverse events such as myelosuppression and neuropathy.
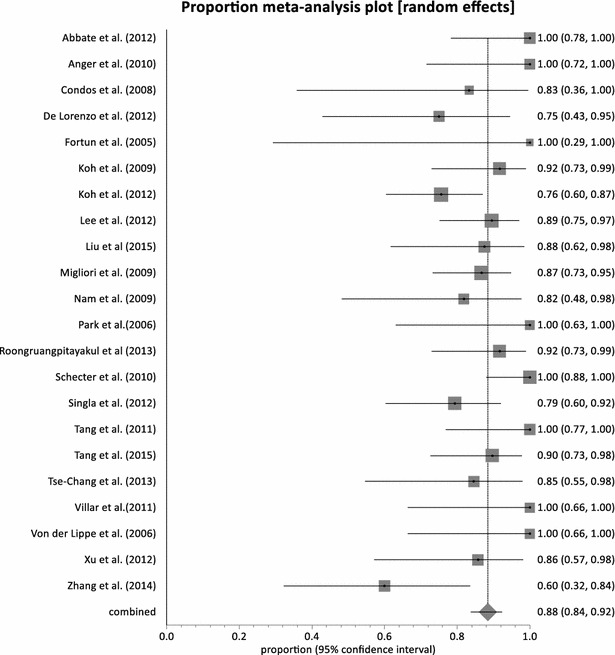
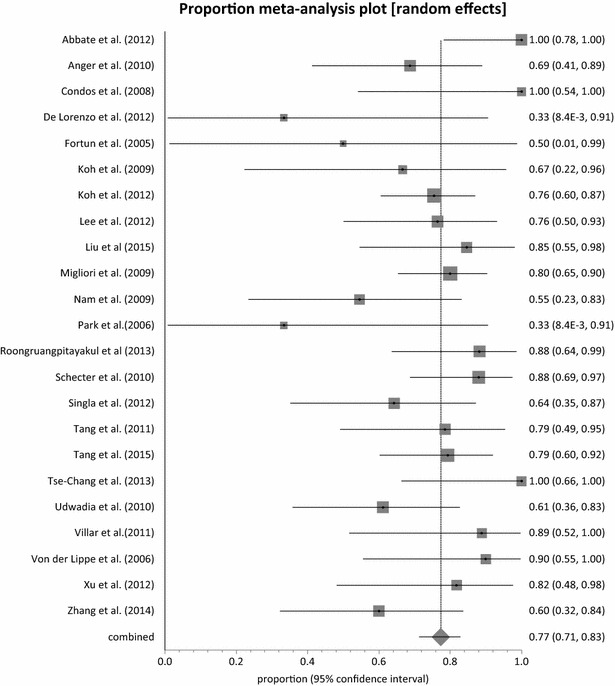
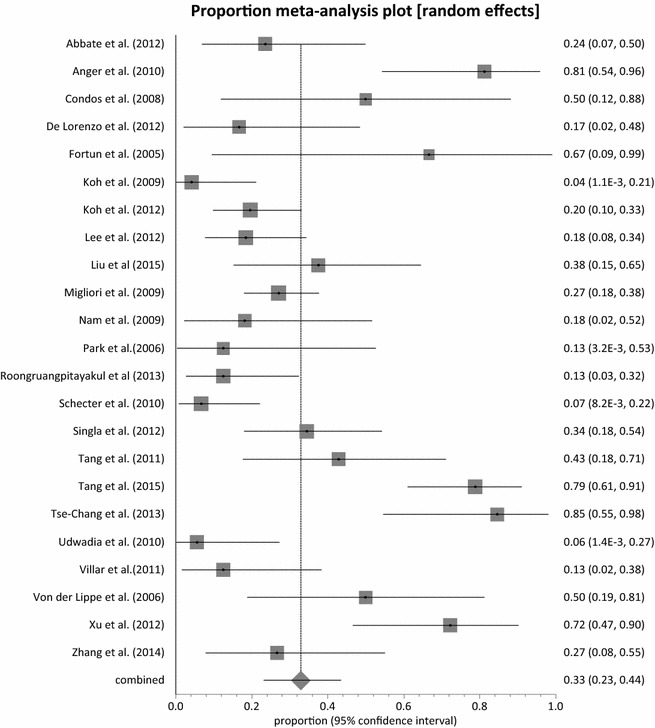
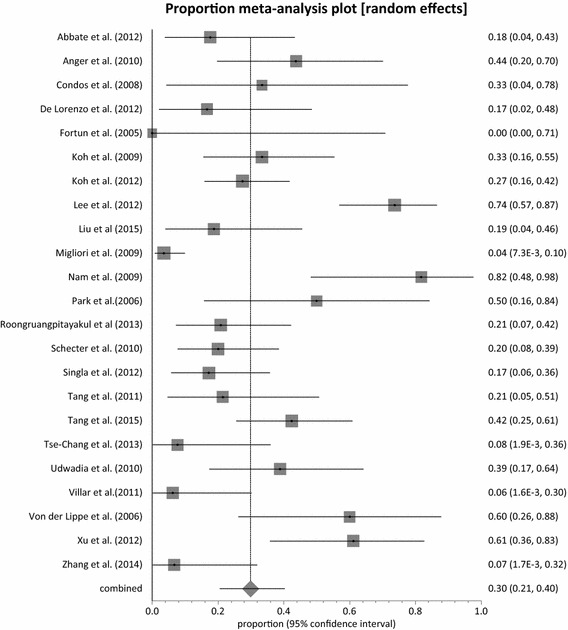
Twenty-three (23) studies conducted in fourteen (14) countries and involving 507 patients were retrieved. Only 1 randomized controlled trial was identified and none of the identified studies involved participants from Africa. The pooled proportion for treatment success was 77.36 % (95 % CI = 71.38-82.83 %, I(2) = 37.6 %) with culture conversion rate determined as 88.45 % (95 % CI = 83.82-92.38 %, I(2) = 45.4 %). There was no strong evidence for both culture conversion (p = 0.0948) and treatment success (p = 0.0695) between linezolid daily doses ≤ 600 and > 600 mg. Only myelosuppression showed a strong statistical significance (p < 0.0001) between dose comparisons. The incidence of neuropathy and other adverse events leading to permanent discontinuation of linezolid also showed no significance upon dose comparisons (p = 0.3213, p = 0.9050 respectively).
Available evidence presents Linezolid as a viable option in the treatment of MDR/XDR TB although patients ought to be monitored closely for the incidence of major adverse events such as myelosuppression and neuropathy. Additionally, highly powered randomized controlled trials including participants from endemic regions are urgently needed to better inform the magnitude and significance of Linezolid treatment effect in MDR and XDR TB patients.
耐多药结核病的治疗选择仍然有限。利奈唑胺已被推荐用于治疗耐多药(MDR)或广泛耐药(XDR)结核病患者,尽管在这些情况下其安全性和耐受性仍存在不确定性。
系统评价利奈唑胺治疗MDR或XDR结核病的疗效和耐受性的现有证据。
我们按照PRISMA指南进行了系统评价和荟萃分析。在PubMed、科学网和EMBASE中进行检索,随后直接检索《国际结核病和肺部疾病杂志》的摘要,以检索2000年1月至2016年1月期间发表的评估利奈唑胺治疗耐药结核病疗效和安全性的原始研究。我们评估了包括培养转阴、治疗成功以及骨髓抑制和神经病变等不良事件发生率等结局的发生情况。
检索到在14个国家开展的23项研究,涉及507例患者。仅识别出1项随机对照试验,且所有识别出的研究均未纳入来自非洲的参与者。治疗成功的合并比例为77.36%(95%CI=71.38-82.83%,I²=37.6%),培养转阴率为88.45%(95%CI=83.82-92.38%,I²=45.4%)。利奈唑胺每日剂量≤600mg与>600mg之间,在培养转阴(p=0.0948)和治疗成功(p=0.0695)方面均无有力证据。仅骨髓抑制在剂量比较中显示出很强的统计学显著性(p<0.0001)。神经病变和导致利奈唑胺永久停药的其他不良事件的发生率在剂量比较中也无显著性(分别为p=0.3213,p=0.9050)。
现有证据表明利奈唑胺是治疗MDR/XDR结核病的一个可行选择,尽管应对患者密切监测骨髓抑制和神经病变等主要不良事件的发生率。此外,迫切需要开展纳入流行地区参与者的大规模随机对照试验,以更好地了解利奈唑胺对MDR和XDR结核病患者的治疗效果的程度和意义。