Department of Child and Adolescent Psychiatry, Hospital General Universitario Gregorio Marañón, CIBERSAM, IiSGM, School of Medicine, Universidad Complutense de Madrid , Madrid, Spain.
Department of Child and Adolescent Psychiatry, Hospital General Universitario Gregorio Marañón, CIBERSAM, IiSGM, School of Medicine, Universidad Complutense de Madrid, Madrid, Spain; Department of Child and Adolescent Psychiatry, Institute of Psychiatry, King's College London, London, UK.
NPJ Schizophr. 2015 Mar 4;1:14005. doi: 10.1038/npjschz.2014.5. eCollection 2015.
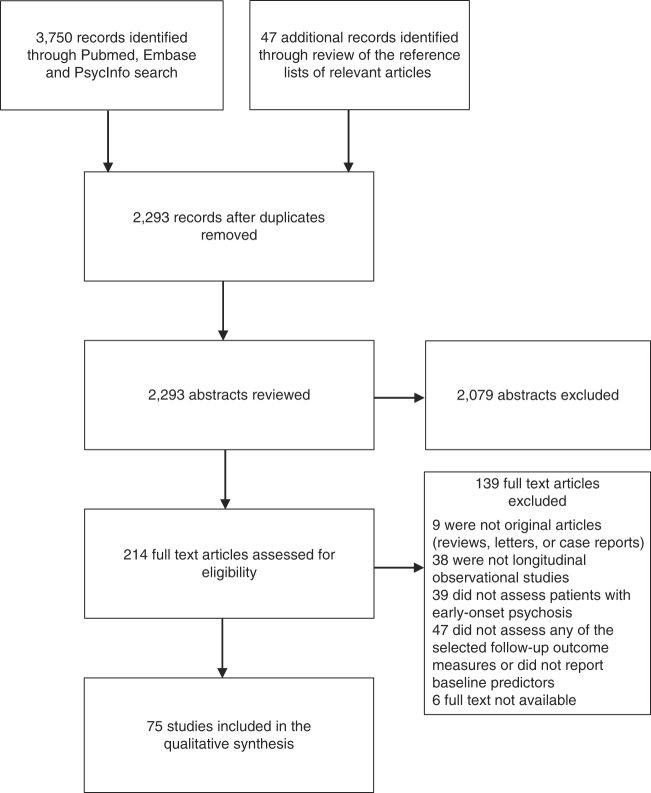
Given the global burden of psychotic disorders, the identification of patients with early-onset psychosis (EOP; that is, onset before the age of 18) at higher risk of adverse outcome should be a priority. A systematic search of Pubmed, Embase, and PsycInfo (1980 through August 2014) was performed to identify longitudinal observational studies assessing correlates and/or predictors of clinical, functional, cognitive, and biological outcomes in EOP. Seventy-five studies were included in the review. Using multivariate models, the most replicated predictors of worse clinical, functional, cognitive, and biological outcomes in EOP were premorbid difficulties and symptom severity (especially of negative symptoms) at baseline. Longer duration of untreated psychosis (DUP) predicted worse clinical, functional, and cognitive outcomes. Higher risk of attempting suicide was predicted by greater severity of psychotic illness and of depressive symptoms at the first episode of psychosis. Age at onset and sex were not found to be relevant predictors of outcome in most multivariate models, whereas studies using bivariate analyses yielded inconsistent results. Lower intelligence quotient at baseline predicted lower insight at follow-up, worse functional outcomes, and a diagnostic outcome of schizophrenia. Biological predictors of outcome in EOP have been little studied and have not been replicated. Lower levels of antioxidants at baseline predicted greater brain volume changes and worse cognitive functioning at follow-up, whereas neuroimaging markers such as regional cortical thickness and gray matter volume at baseline predicted remission and better insight at follow-up, respectively. EOP patients with poorer premorbid adjustment and prominent negative symptoms at initial presentation are at risk of poor outcome. They should therefore be the target of careful monitoring and more intensive interventions to address whether the disease course can be modified in this especially severely affected group. Early intervention strategies to reduce DUP may also improve outcome in EOP.
鉴于精神疾病在全球的负担,识别有较高不良预后风险的早发性精神病(EOP;即发病年龄在 18 岁之前)患者应成为优先事项。系统检索了 Pubmed、Embase 和 PsycInfo(1980 年至 2014 年 8 月),以确定评估 EOP 患者临床、功能、认知和生物学结局的相关性和/或预测因素的纵向观察性研究。有 75 项研究被纳入综述。使用多变量模型,EOP 患者预后更差的临床、功能、认知和生物学预测因子是发病前的困难和基线时的症状严重程度(特别是阴性症状)。未治疗精神病持续时间(DUP)较长预测临床、功能和认知结局较差。首次精神病发作时精神病严重程度和抑郁症状越严重,自杀风险越高。在大多数多变量模型中,发病年龄和性别都不是相关的预后预测因子,而使用双变量分析的研究得出的结果不一致。基线时的智商较低预测随访时的洞察力较低、功能结局较差和精神分裂症的诊断结果。EOP 患者的生物学预后预测因素研究较少,也未得到复制。基线时的抗氧化剂水平较低预测随访时的大脑体积变化较大和认知功能较差,而基线时的神经影像学标志物,如区域皮质厚度和灰质体积,分别预测随访时的缓解和更好的洞察力。初次就诊时表现出较差的发病前调整和明显的阴性症状的 EOP 患者有预后不良的风险。因此,他们应该是仔细监测和更强化干预的目标,以确定是否可以改变这群特别受影响的患者的疾病进程。减少 DUP 的早期干预策略也可能改善 EOP 的结局。