Ni Yang, Bi Jingwang, Ye Xin, Fan Weijun, Yu Guohua, Yang Xia, Huang Guanghui, Li Wenhong, Wang Jiao, Han Xiaoying, Ni Xiang, Wei Zhigang, Han Mingyong, Zheng Aimin, Meng Min, Xue Guoliang, Zhang Liang, Wan Chao
Department of Oncology, Shandong Provincial Hospital Affiliated to Shandong University Department of Oncology, Jinan Military General Hospital of Chinese People's Liberation Army Imaging and Interventional Center, Sun Yat-sen University Cancer Center Department of Oncology, Weifang People's Hospital Affiliated to Weifang Medical University, China.
Medicine (Baltimore). 2016 Jun;95(25):e3998. doi: 10.1097/MD.0000000000003998.
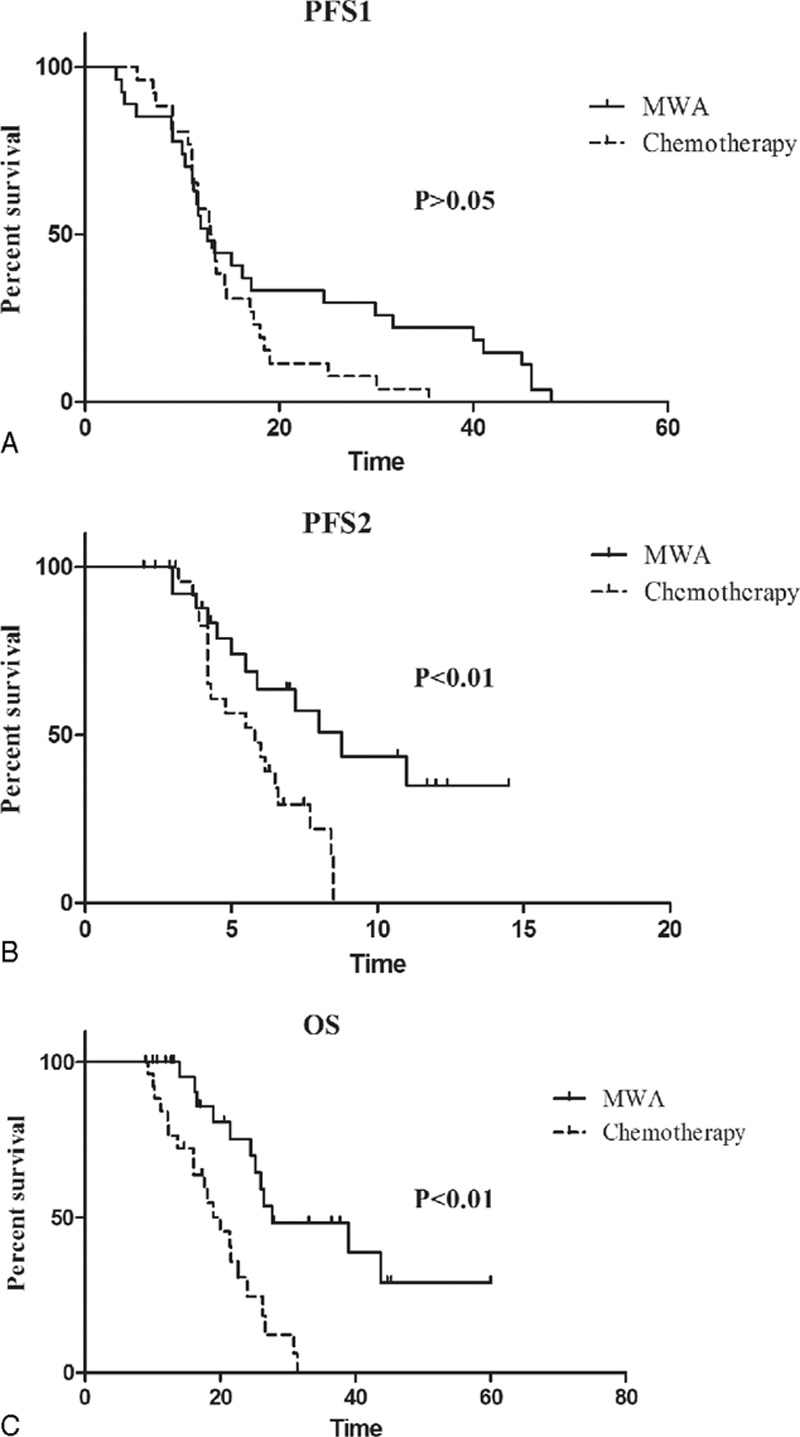
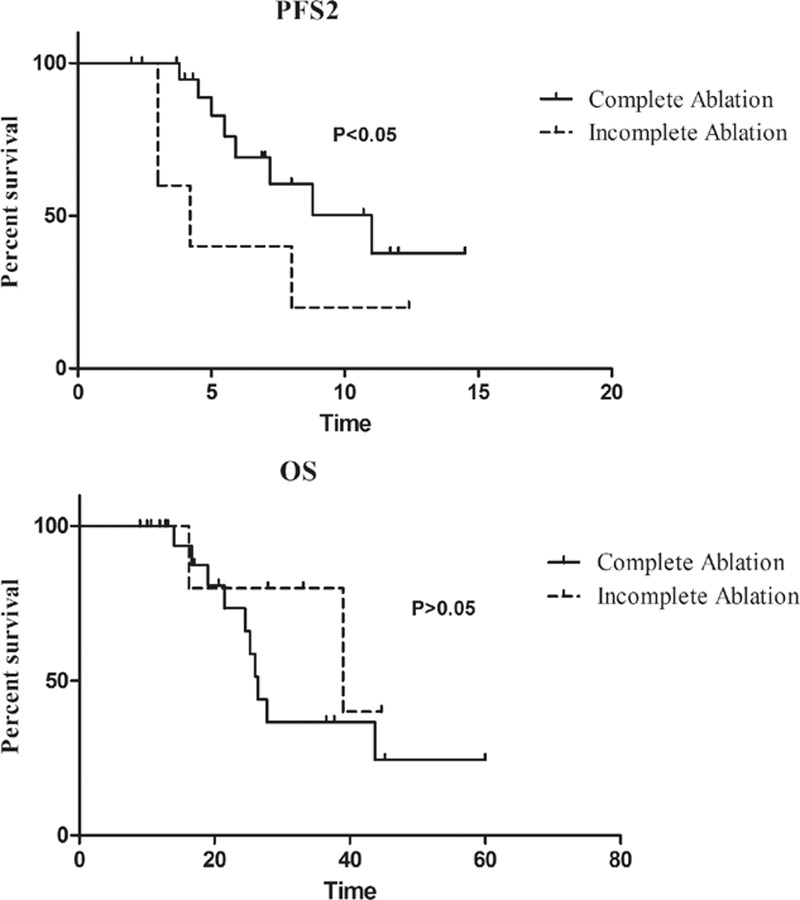
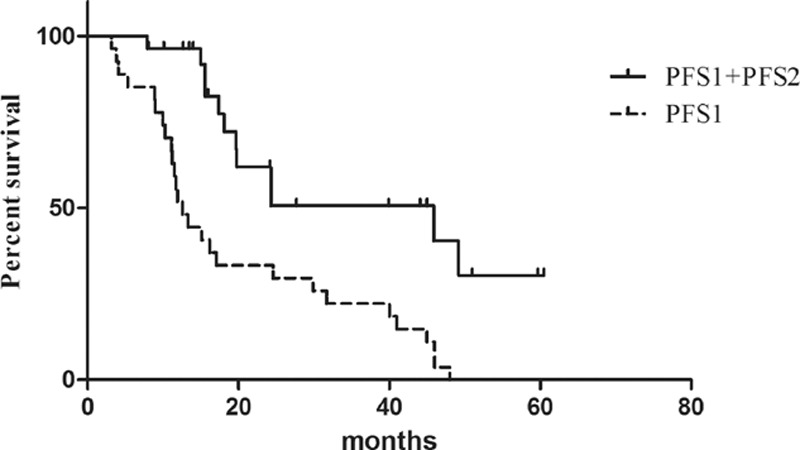
The non-small cell lung cancer (NSCLC) patients that experienced good clinical response to epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKIs) will ultimately develop acquired resistance. This retrospective study was performed to explore the potential survival benefit of microwave ablation (MWA) therapy in epidermal growth factor receptor (EGFR)-mutant NSCLC that developed extra-central nervous system (CNS) oligoprogressive disease during TKI treatment.We retrospectively analyzed 54 NSCLC patients with EGFR mutations who showed a clinical benefit from initial EGFR-TKI therapy and developed extra-CNS oligoprogressive disease at our institutions. Twenty eight patients received MWA as a local therapy for the metastatic sites and continued on the same TKIs (MWA group). The following 26 patients received systemic chemotherapy after progression (chemotherapy group). The progression-free survival (PFS1) was calculated from initiation of targeted therapy to first progression. Progression-free survival (PFS2) was defined from first progression to second progression after MWA or chemotherapy. Overall survival (OS) was calculated from the time of diagnosis to the date of last follow-up or death.The median PFS1 for both groups was similar (median 12.6 vs. 12.9 months, HR 0.63). However, the MWA group patients had a significantly longer PFS2 (median 8.8 vs. 5.8 months, hazards ratio [HR] 0.357) and better OS (median 27.7 vs. 20.0, HR 0.238) in comparison with chemotherapy group. Multivariate analysis and the internal validation identified MWA as the main favorable prognostic factor for PFS2 and OS. In the MWA group, the median PFS2 for complete ablation was significantly longer than that for incomplete ablation (11 vs. 4.2 months, HR 0.29, P < 0.05).MWA with continued EGFR inhibition might be associated with favorable progression-free survival (PFS) and OS in patients with extra-CNS oligometastatic disease. MWA as a local therapy for extra-CNS oligometastatic disease should be considered for NSCLC with acquired resistance to EGFR-TKIs.
对表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKIs)产生良好临床反应的非小细胞肺癌(NSCLC)患者最终会产生获得性耐药。本回顾性研究旨在探讨微波消融(MWA)治疗在TKI治疗期间发生中枢神经系统(CNS)外寡进展性疾病的表皮生长因子受体(EGFR)突变NSCLC患者中的潜在生存获益。我们回顾性分析了54例在我院接受初始EGFR-TKI治疗后出现临床获益且发生CNS外寡进展性疾病的EGFR突变NSCLC患者。28例患者接受MWA作为转移部位的局部治疗,并继续使用相同的TKI(MWA组)。接下来的26例患者在疾病进展后接受全身化疗(化疗组)。无进展生存期(PFS1)从靶向治疗开始计算至首次进展。无进展生存期(PFS2)定义为MWA或化疗后从首次进展至第二次进展。总生存期(OS)从诊断时间计算至最后一次随访或死亡日期。两组的中位PFS1相似(中位12.6个月对12.9个月,HR 0.63)。然而,与化疗组相比,MWA组患者的PFS2显著更长(中位8.8个月对5.8个月,风险比[HR] 0.357),OS更好(中位27.7个月对20.0个月,HR 0.238)。多因素分析和内部验证确定MWA是PFS2和OS的主要有利预后因素。在MWA组中,完全消融的中位PFS2显著长于不完全消融(11个月对4.2个月,HR 0.29,P<0.05)。持续抑制EGFR的MWA可能与CNS外寡转移疾病患者良好的无进展生存期(PFS)和总生存期(OS)相关。对于对EGFR-TKIs产生获得性耐药的NSCLC患者,应考虑将MWA作为CNS外寡转移疾病的局部治疗方法。