Feldman Anna Z, Brown Florence M
Joslin Diabetes Center, 1 Joslin Place, Boston, MA, 02115, USA.
Curr Diab Rep. 2016 Aug;16(8):76. doi: 10.1007/s11892-016-0765-z.
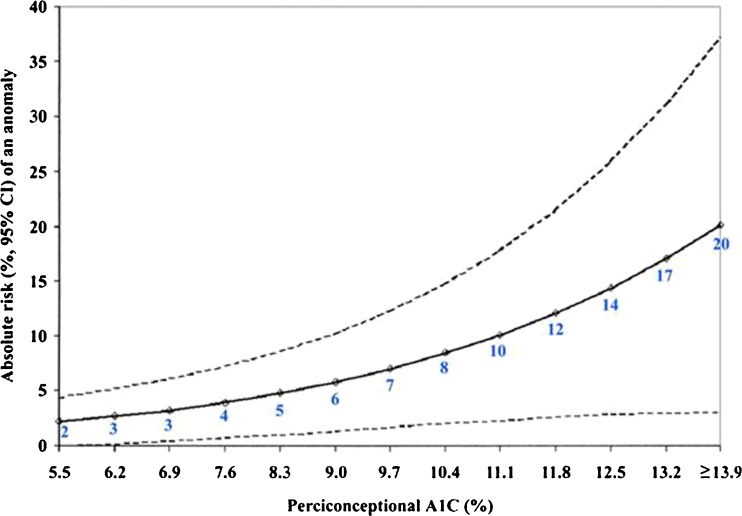
Women with type 1 diabetes (T1DM) have unique needs during the preconception, pregnancy, and postpartum periods. Preconception counseling is essential for women with T1DM to minimize pregnancy risks. The goals of preconception care should be tight glycemic control with a hemoglobin A1c (A1C) < 7 % and as close to 6 % as possible, without significant hypoglycemia. This will lower risks of congenital malformations, preeclampsia, and perinatal mortality. The safety of medications should be assessed prior to conception. Optimal control of retinopathy, hypertension, and nephropathy should be achieved. During pregnancy, the goal A1C is near-normal at <6 %, without excessive hypoglycemia. There is no clear evidence that continuous subcutaneous insulin infusion (CSII) versus multiple daily injections (MDI) is superior in achieving the desired tight glycemic control of T1DM during pregnancy. Data regarding continuous glucose monitoring (CGM) in pregnant women with T1DM is conflicting regarding improved glycemic control. However, a recent CGM study does provide some distinct patterns of glucose levels associated with large for gestational age infants. Frequent eye exams during pregnancy are essential due to risk of progression of retinopathy during pregnancy. Chronic hypertension treatment goals are systolic blood pressure 110-129 mmHg and diastolic blood pressure 65-79 mmHg. Labor and delivery target plasma glucose levels are 80-110 mg/dl, and an insulin drip is recommended to achieve these targets during active labor. Postpartum, insulin doses must be reduced and glucoses closely monitored in women with T1DM because of the enhanced insulin sensitivity after delivery. Breastfeeding is recommended and should be highly encouraged due to maternal benefits including increased insulin sensitivity and weight loss and infant and childhood benefits including reduced prevalence of overweight. In this article, we discuss the care of pregnant patients with T1DM.
1型糖尿病(T1DM)女性在孕前、孕期及产后有独特的需求。孕前咨询对T1DM女性至关重要,可将妊娠风险降至最低。孕前护理的目标应是严格控制血糖,糖化血红蛋白(A1C)<7%,并尽可能接近6%,同时避免严重低血糖。这将降低先天性畸形、子痫前期和围产期死亡率的风险。受孕前应评估药物安全性。应实现视网膜病变、高血压和肾病的最佳控制。孕期A1C的目标是接近正常水平,即<6%,且无过度低血糖。没有明确证据表明,在孕期实现T1DM所需的严格血糖控制方面,持续皮下胰岛素输注(CSII)优于多次皮下注射(MDI)。关于T1DM孕妇连续血糖监测(CGM)在改善血糖控制方面的数据存在矛盾。然而,最近一项CGM研究确实提供了一些与大于胎龄儿相关的独特血糖水平模式。由于孕期视网膜病变有进展风险,孕期频繁进行眼科检查至关重要。慢性高血压的治疗目标是收缩压110 - 129 mmHg,舒张压65 - 79 mmHg。分娩时目标血浆葡萄糖水平为80 - 110 mg/dl,建议在活跃分娩期使用胰岛素静脉滴注来达到这些目标。产后,由于分娩后胰岛素敏感性增强,T1DM女性必须减少胰岛素剂量并密切监测血糖。建议母乳喂养,并且应大力鼓励,因为母乳喂养对母亲有益,包括增加胰岛素敏感性和体重减轻,对婴儿和儿童也有益,包括降低超重患病率。在本文中,我们讨论了T1DM孕妇的护理。