Liu Qianwen, Gu Zhitao, Yang Fu, Fu Jianhua, Shen Yi, Wei Yucheng, Tan Lijie, Zhang Peng, Han Yongtao, Chen Chun, Zhang Renquan, Li Yin, Chen Ke-Neng, Chen Hezhong, Liu Yongyu, Cui Youbing, Wang Yun, Pang Liewen, Yu Zhentao, Zhou Xinming, Liu Yangchun, Xiang Jin, Liu Yuan, Fang Wentao
Department of Thoracic Surgery, Guangdong Esophageal Cancer Institute, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center of Cancer Medicine, Guangzhou 510060, China.
Department of Thoracic Surgery, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai 200030, China.
Zhongguo Fei Ai Za Zhi. 2016 Jul 20;19(7):465-72. doi: 10.3779/j.issn.1009-3419.2016.07.09.
Postoperative radiotherapy (PORT) for thymic tumor is still controversial. The object of the study is to evaluate the role of PORT for stage I/II/III thymic tumor.
The database of Chinese Alliance of Research for Thymomas (ChART) was retrieved for patients with stage I/II/III thymic tumor who underwent surgical therapy without neoajuvant therapy between 1994 and 2012. Univariate and multivariate survival analyses were performed. Cox proportional hazard model was used to determine the hazard ratio for death.
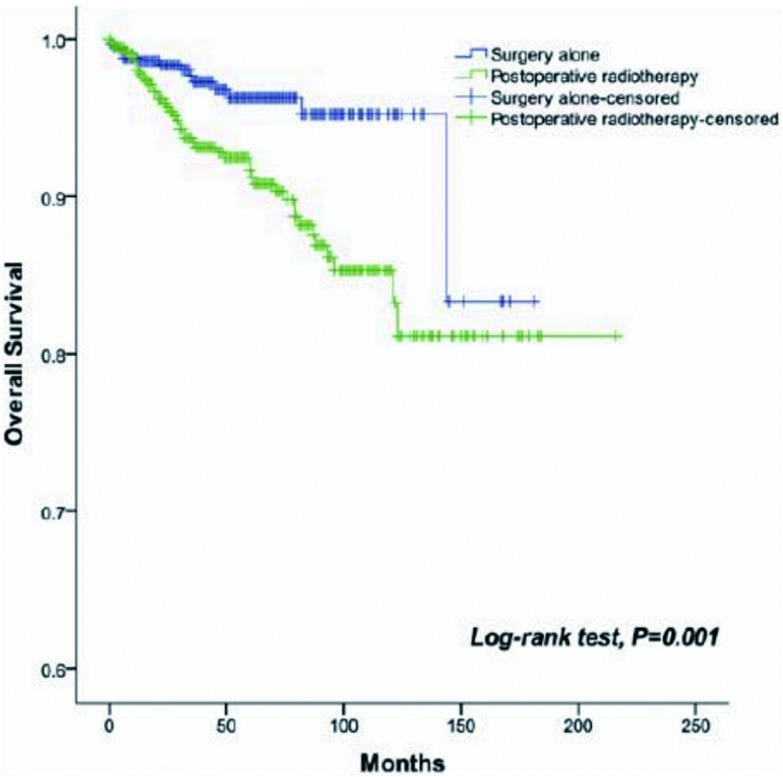
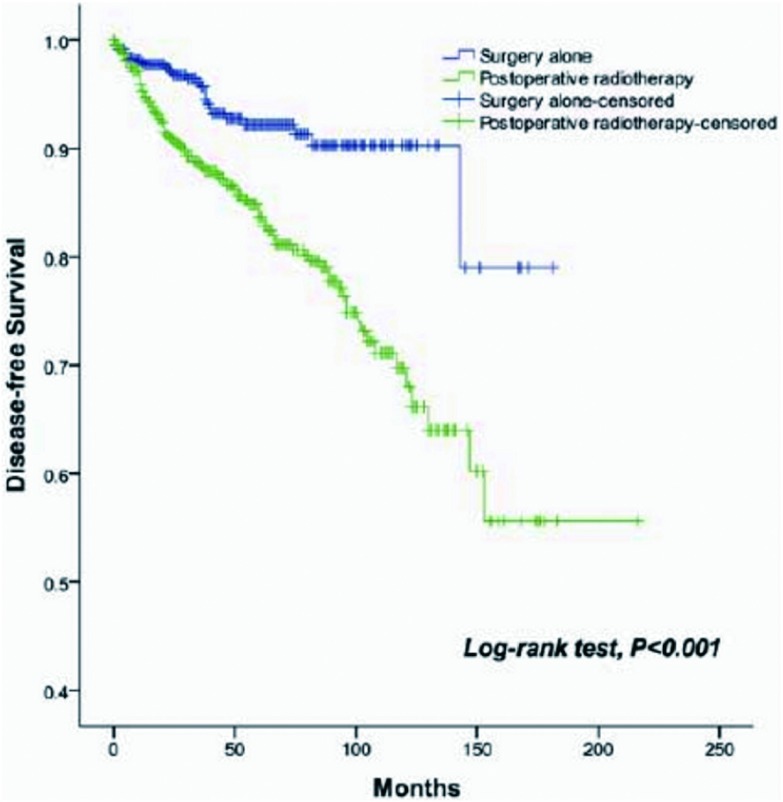
1,546 stage I/II/III patients were identified from ChART database. Among these patients, 649 (41.98%) underwent PORT. PORT was associated with gender, histologic type (World Health Organization, WHO), surgical extent, complete resection, Masaoka stage and adjuvant chemotherapy. The 5-yr and 10-yr overall survival (OS) rates and disease-free survival (DFS) rate for patients underwent surgery followed by PORT were 90% and 80%, 81% and 63%, comparing with 96% and 95%, 92% and 90% for patients underwent surgery alone (P=0.001, P<0.001) respectively. In univariate analysis, age, histologic type (WHO), Masaoka stage, completeness of resection, and PORT were associated with OS. Multivariable analysis showed that histologic type (WHO)(P=0.001), Masaoka stage (P=0.029) and completeness of resection (P=0.003) were independently prognostic factors of OS. In univariate analysis, gender, myasthenia gravis, histologic type (WHO), Masaoka stage, surgical approach, PORT and completeness of resection were associated with DFS. Multivariable analysis showed that histologic type (WHO) (P<0.001), Masaoka stage (P=0.005) and completeness of resection (P=0.006) were independently prognostic factors of DFS. Subgroup analysis showed that patients with incomplete resection underwent PORT achieved the better OS and DFS (P=0.010, 0.017, respectively). However, patients with complete resection underwent PORT had the worse OS and DFS (P<0.001, P<0.001, respectively).
CONCLUSIONS: The current retrospective study indicated that PORT after incomplete resection could improve OS and DFS for patients with stage I/II/III thymic tumor. But for those after complete resection, PORT may not help improve prognosis on the whole. .
胸腺肿瘤术后放疗(PORT)仍存在争议。本研究的目的是评估PORT在Ⅰ/Ⅱ/Ⅲ期胸腺肿瘤中的作用。
检索中国胸腺瘤研究联盟(ChART)数据库,纳入1994年至2012年间接受手术治疗且未接受新辅助治疗的Ⅰ/Ⅱ/Ⅲ期胸腺肿瘤患者。进行单因素和多因素生存分析。采用Cox比例风险模型确定死亡风险比。
从ChART数据库中识别出1546例Ⅰ/Ⅱ/Ⅲ期患者。其中,649例(41.98%)接受了PORT。PORT与性别、组织学类型(世界卫生组织,WHO)、手术范围、完整切除、Masaoka分期及辅助化疗相关。接受手术加PORT的患者5年和10年总生存率(OS)及无病生存率(DFS)分别为90%和80%、81%和63%,而单纯接受手术的患者分别为96%和95%、92%和90%(P=0.001,P<0.001)。单因素分析显示,年龄、组织学类型(WHO)、Masaoka分期、切除完整性及PORT与OS相关。多因素分析表明,组织学类型(WHO)(P=0.001)、Masaoka分期(P=0.029)及切除完整性(P=0.003)是OS的独立预后因素。单因素分析显示,性别、重症肌无力、组织学类型(WHO)、Masaoka分期、手术方式、PORT及切除完整性与DFS相关。多因素分析表明,组织学类型(WHO)(P<0.001)、Masaoka分期(P=0.005)及切除完整性(P=0.006)是DFS的独立预后因素。亚组分析显示,切除不完整的患者接受PORT后OS和DFS更佳(分别为P=0.010,0.017)。然而,切除完整的患者接受PORT后OS和DFS更差(分别为P<0.001,P<0.001)。
当前的回顾性研究表明,Ⅰ/Ⅱ/Ⅲ期胸腺肿瘤患者切除不完整后行PORT可改善OS和DFS。但对于切除完整的患者,PORT总体上可能无助于改善预后。