Melamed Nir, Pittini Alex, Hiersch Liran, Yogev Yariv, Korzeniewski Steven J, Romero Roberto, Barrett Jon
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Sunnybrook Health Sciences Center, University of Toronto, Toronto, Ontario, Canada.
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Sunnybrook Health Sciences Center, University of Toronto, Toronto, Ontario, Canada.
Am J Obstet Gynecol. 2016 Nov;215(5):616.e1-616.e14. doi: 10.1016/j.ajog.2016.06.034. Epub 2016 Jun 27.
Cervical length at midtrimester is a powerful predictor of preterm birth in twin gestations. However, given the fact that, in some cases, cervical shortening may become evident only later during the second trimester, it seems reasonable that serial monitoring of cervical length may improve the detection of preterm birth in women with twins. However, data in support of such a practice are limited and conflicting. The contradictory results may be related to the fact that in most of these studies, the analysis of the predictive value of serial measurements of cervical length was limited to data derived from only two sequential measurements of cervical length, while data on the predictive value of multiple (>2) measurements are scarce.
We sought to determine whether serial measurements of cervical length can improve the prediction of preterm birth in asymptomatic women with twin gestations compared with a single measurement of cervical length at midgestation.
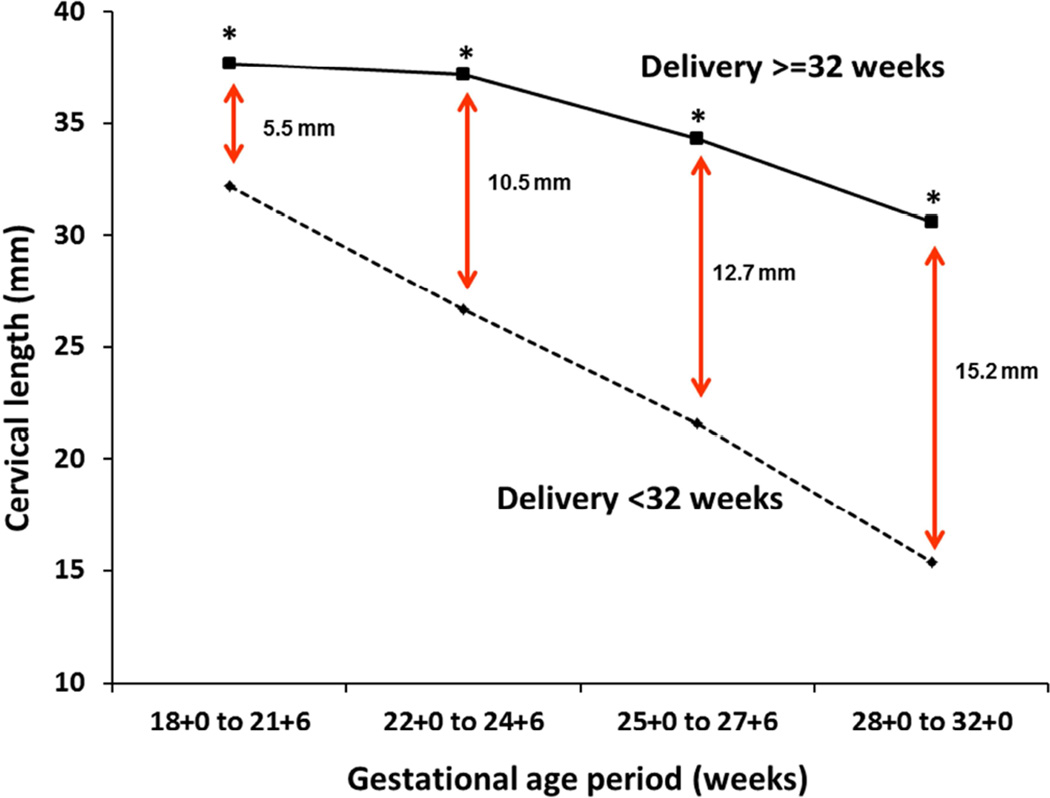
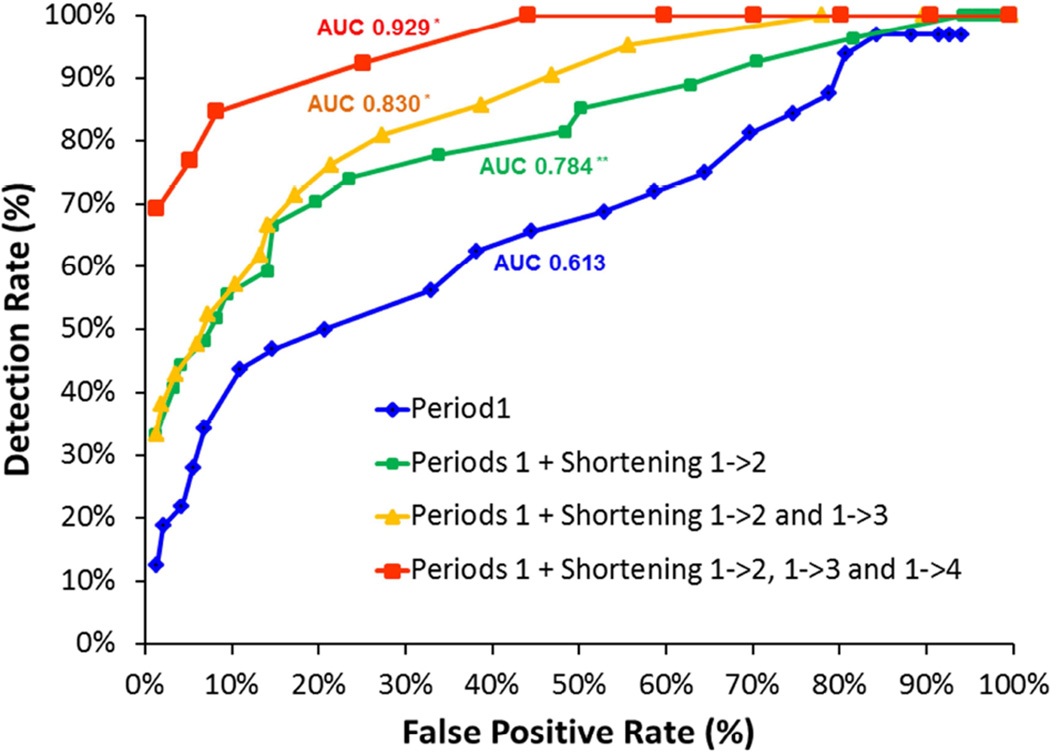
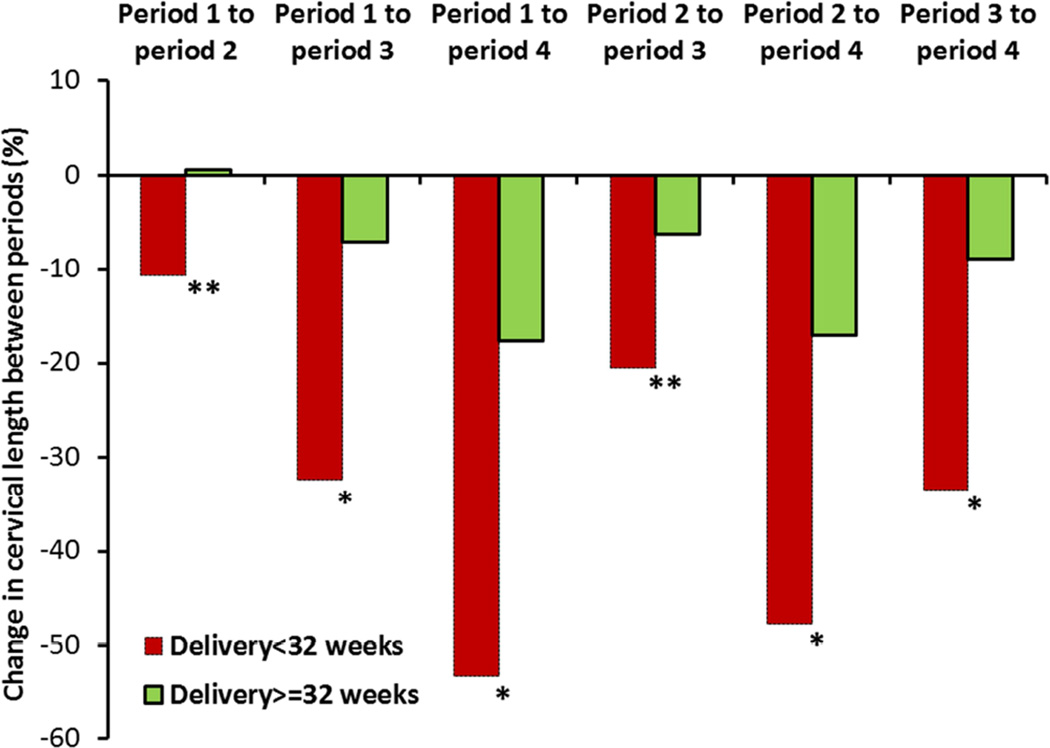
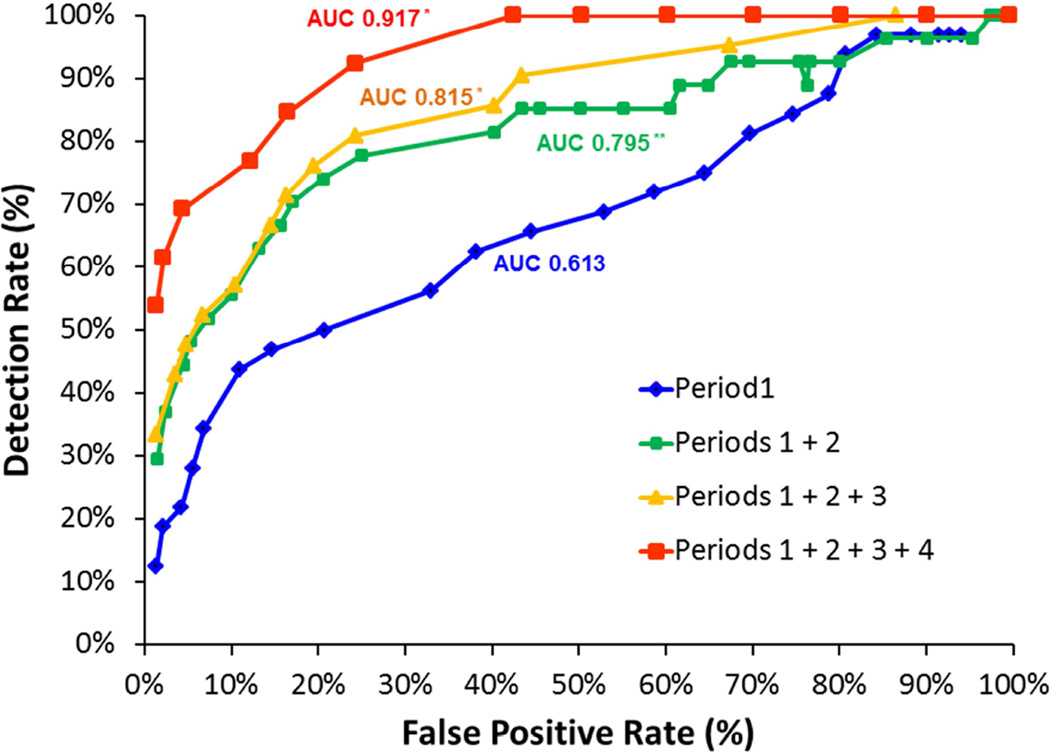
This was a retrospective cohort study of women with twin pregnancies followed up in a tertiary medical center from 2012 through 2014. All participants underwent routine measurement of cervical length at midgestation and every 2-3 weeks thereafter until 28-32 weeks. For each patient, cervical length was determined at the following time periods: 18+0 to 21+6 weeks (period 1, routine exam), 22+0 to 24+6 weeks (period 2), 25+0 to 27+6 weeks (period 3), and 28+0 to 32+0 weeks (period 4). Measurements of cervical length at periods 2-4 were analyzed in the form of either absolute length (in millimeters) or percent shortening relative to cervical length at period 1. The performance of a stepwise algorithm that incorporated serial measurements of cervical length for the prediction of preterm birth was compared to that achieved with a single measurement of cervical length at period 1.
Overall, 441 women with twin pregnancies who were eligible for the study underwent a total of 2374 cervical length measurements. The association of a short cervix (<10th percentile) with preterm birth at <32 weeks persisted in each of the 4 periods of gestation [odds ratio (95% confidence interval): 7.2 (3.1-16.5), 15.3 (6.4-36.7), 10.3 (4.4-24.3), and 23.1(8.3-64.1), respectively]. Compared with a single measurement of cervical length at midgestation (period 1), a stepwise algorithm integrating serial cervical length measurements from all 4 successive gestational age periods resulted in a significant increase in the area under the receiver operating characteristic curve (0.917 vs 0.613, P < .001). Similarly, when a target false-positive rate of 5% was used, the same stepwise algorithm was associated with a higher detection rate (69% vs 28%, P < .001), higher positive likelihood ratio (14.54 vs 5.12), and lower negative likelihood ratio (0.32 vs 0.76) for preterm birth at <32 weeks compared with a single measurement of cervical length at period 1.
Integration of serial measurements of cervical length using a stepwise algorithm in asymptomatic women with twin gestations can improve the detection of women at risk of preterm birth. Prospective studies are needed to validate these findings, and to investigate whether improved risk assessment performance is sufficient to offset the additional costs associated with serial cervical length measurements.
孕中期宫颈长度是双胎妊娠早产的有力预测指标。然而,鉴于在某些情况下,宫颈缩短可能仅在孕中期后期才变得明显,对宫颈长度进行连续监测可能会提高双胎妊娠妇女早产的检出率,这似乎是合理的。然而,支持这种做法的数据有限且相互矛盾。矛盾的结果可能与以下事实有关:在大多数这些研究中,宫颈长度连续测量的预测价值分析仅限于仅来自宫颈长度的两次连续测量的数据,而关于多次(>2次)测量的预测价值的数据很少。
我们试图确定与孕中期单次测量宫颈长度相比,连续测量宫颈长度是否能改善无症状双胎妊娠妇女早产的预测。
这是一项对2012年至2014年在三级医疗中心接受随访的双胎妊娠妇女的回顾性队列研究。所有参与者在孕中期接受宫颈长度的常规测量,此后每2-3周测量一次,直至孕28-32周。对于每位患者,在以下时间段确定宫颈长度:18+0至21+6周(第1期,常规检查)、22+0至24+6周(第2期)、25+0至27+6周(第3期)和28+0至32+0周(第4期)。第2-4期宫颈长度的测量以绝对长度(毫米)或相对于第1期宫颈长度的缩短百分比的形式进行分析。将纳入宫颈长度连续测量以预测早产的逐步算法的性能与第1期单次测量宫颈长度的性能进行比较。
总体而言,441例符合研究条件的双胎妊娠妇女共进行了2374次宫颈长度测量。宫颈短(<第10百分位数)与孕32周前早产的关联在妊娠的4个时期中均持续存在[比值比(95%置信区间):分别为7.2(3.1-16.5)、15.3(6.4-36.7)、10.3(4.4-24.3)和23.1(8.3-64.1)]。与孕中期(第1期)单次测量宫颈长度相比,整合所有4个连续孕周时期的宫颈长度连续测量的逐步算法导致受试者操作特征曲线下面积显著增加(0.917对0.613,P<.001)。同样,当使用5%的目标假阳性率时,与第1期单次测量宫颈长度相比,相同的逐步算法与孕32周前早产的更高检出率(69%对28%,P<.001)、更高的阳性似然比(14.54对5.12)和更低的阴性似然比(0.32对0.76)相关。
在无症状双胎妊娠妇女中使用逐步算法整合宫颈长度的连续测量可以提高早产风险妇女的检出率。需要进行前瞻性研究来验证这些发现,并调查改善的风险评估性能是否足以抵消与宫颈长度连续测量相关的额外成本。