de Boysson Hubert, Liozon Eric, Lambert Marc, Parienti Jean-Jacques, Artigues Nicolas, Geffray Loïk, Boutemy Jonathan, Ollivier Yann, Maigné Gwénola, Ly Kim, Huglo Damien, Hachulla Eric, Hatron Pierre-Yves, Aouba Achille, Manrique Alain, Bienvenu Boris
aDepartment of Internal Medicine, Caen University Hospital, Basse-Normandie University bDepartment of Internal Medicine, Limoges University Hospital cDepartment of Internal Medicine, Lille University Hospital dBiostatistics and Clinical Research Unit, Caen University Hospital eDepartment of Internal Medicine, Bayeux Hospital fDepartment of Internal Medicine, Lisieux Hospital gDepartment of Nuclear Medicine, Lille University Hospital hDepartment of Nuclear Medicine, Caen University Hospital, Normandie University France.
Medicine (Baltimore). 2016 Jun;95(26):e3851. doi: 10.1097/MD.0000000000003851.
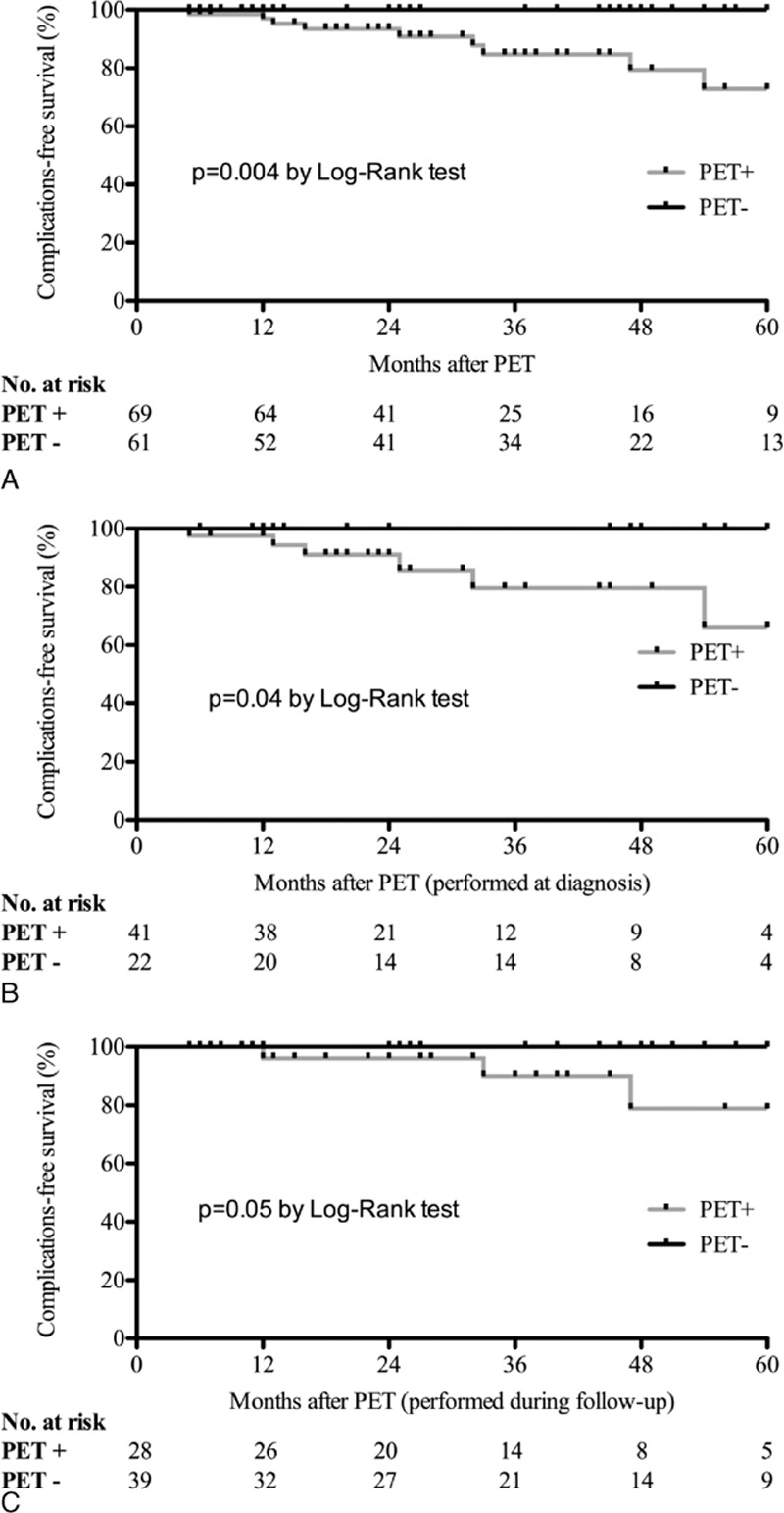
Previous studies reported a 2- to 17-fold higher risk of aortic complications (dilation or dissection) in patients with giant-cell arteritis (GCA). We aimed to determine whether or not GCA patients with large-vessel involvement demonstrated by positron emission tomography with F-fluorodeoxyglucose combined with computed tomography (FDG-PET/CT) have a higher risk of aortic complications. We conducted a retrospective multicenter study between 1995 and 2014. Patients were included if they fulfilled at least 3 American College of Rheumatology criteria for GCA, or 2 criteria associated with extratemporal biopsy-proven giant-cell vasculitis; they underwent at least 1 FDG-PET/CT scan at diagnosis or during follow-up; and the morphology of the aorta was assessed by medical imaging at diagnosis. Patients with an aortic complication at the time of diagnosis were excluded. Of the 130 patients included [85 women (65%), median age 70 (50-86)], GCA was biopsy proven in 77 (59%). FDG-PET/CT was performed at diagnosis in 63 (48%) patients and during the follow-up period in the 67 (52%) remaining patients. FDG-PET/CT was positive in 38/63 (60%) patients at diagnosis and in 31/67 (46%) patients when performed during follow-up (P = NS). One hundred four patients (80%) underwent at least 1 morphological assessment of the aorta during follow-up. Nine (9%) patients developed aortic complications (dilation in all and dissection in 1) at a median time of 33 (6-129) months after diagnosis. All of them displayed large-vessel inflammation on previous FDG-PET/CT. A positive FDG-PET/CT was significantly associated with a higher risk of aortic complications (P = 0.004).In our study, a positive FDG-PET/CT was associated with an increased risk of aortic complications at 5 years.
既往研究报告称,巨细胞动脉炎(GCA)患者发生主动脉并发症(扩张或夹层)的风险要高2至17倍。我们旨在确定,通过氟脱氧葡萄糖正电子发射断层扫描联合计算机断层扫描(FDG-PET/CT)显示有大血管受累的GCA患者发生主动脉并发症的风险是否更高。我们在1995年至2014年间开展了一项回顾性多中心研究。符合以下条件的患者被纳入研究:至少满足美国风湿病学会的3条GCA标准,或满足2条与颞外活检证实的巨细胞血管炎相关的标准;在诊断时或随访期间至少接受过1次FDG-PET/CT扫描;诊断时通过医学成像评估主动脉形态。诊断时即有主动脉并发症的患者被排除。在纳入的130例患者中[85例女性(65%),年龄中位数70岁(50-86岁)],77例(59%)经活检证实为GCA。63例(48%)患者在诊断时进行了FDG-PET/CT检查,其余67例(52%)患者在随访期间进行了该检查。诊断时38/63例(60%)患者的FDG-PET/CT呈阳性,随访期间进行该检查时31/67例(46%)患者呈阳性(P=无显著性差异)。104例(80%)患者在随访期间至少接受过1次主动脉形态学评估。9例(9%)患者在诊断后中位数33个月(6-129个月)出现主动脉并发症(均为扩张,1例为夹层)。所有这些患者既往的FDG-PET/CT均显示有大血管炎症。FDG-PET/CT呈阳性与主动脉并发症风险较高显著相关(P=0.004)。在我们的研究中,FDG-PET/CT呈阳性与5年内主动脉并发症风险增加相关。