Zheng Ninggang, Wei Xiaodong, Zhang Dongzhi, Chai Wenxiao, Che Ming, Wang Jiangye, Du Binbin
aDepartment of Tumor Intervetion Division, Gansu Provincial Hospital, Lanzhou, China bDepartment of Emergency, Gansu Provincial Hospital, Lanzhou, China cDepartment of Anorectal Surgery, Gansu Provincial Hospital, Lanzhou, China.
Medicine (Baltimore). 2016 Jun;95(26):e3959. doi: 10.1097/MD.0000000000003959.
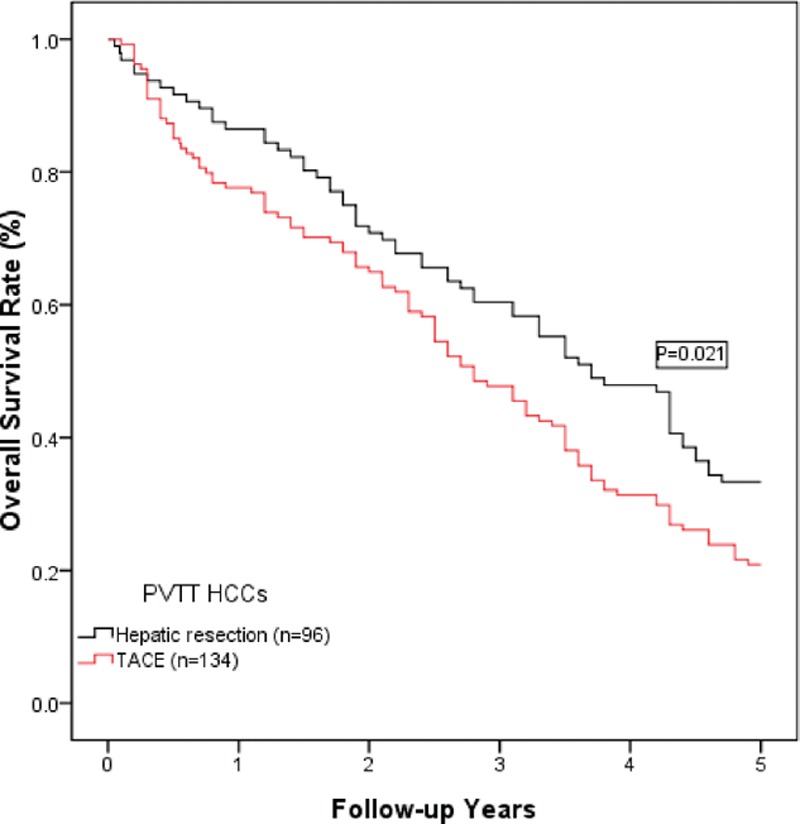
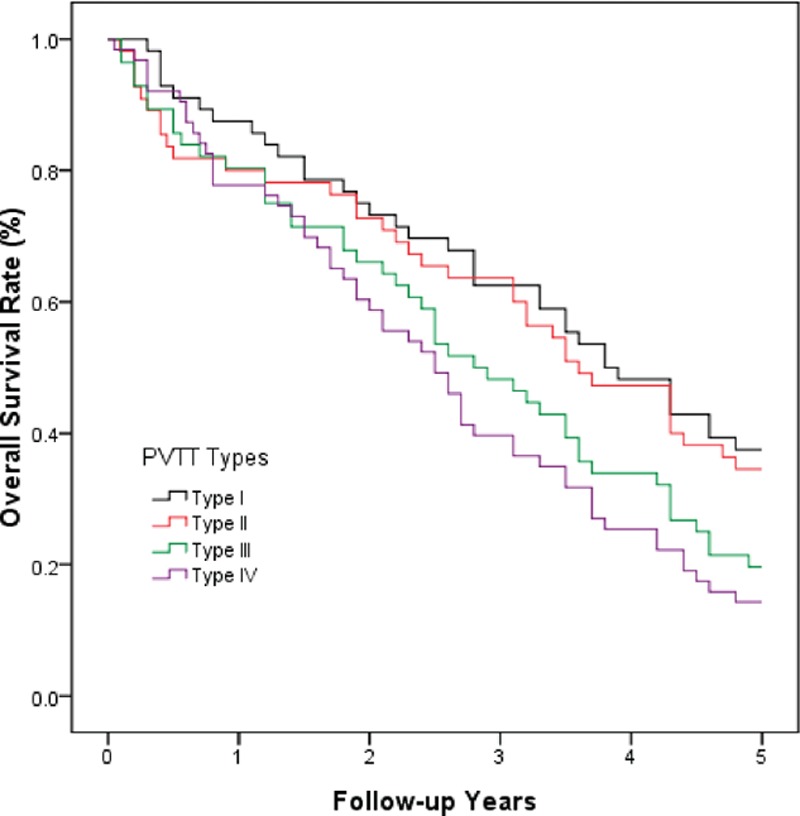
The role of hepatic resection in hepatocellular carcinoma (HCC) with accompanying portal vein tumor thrombus (PVTT) remains controversial. This study aimed to evaluate the surgical outcomes of hepatic resection compared with those of transarterial chemoembolization (TACE) in HCC patients. A retrospective study was conducted using the medical records of 230 HCC patients with portal vein invasion who underwent hepatic resection (96 patients) or TACE (134 patients). The baseline characteristics, tumor characteristics, clinicopathological parameters, and overall survival rates were compared between the 2 groups. The baseline and tumor characteristics were comparable between the hepatic resection and TACE groups. The overall complication rate was 35.4% in the hepatic resection group, which was significantly lower than that in the TACE group (73.0%, P <0.001). However, the serious complication rate (grade ≥3) in the hepatic resection group was 13.5%, which was significantly higher than that in the TACE group (P = 0.003). The cumulative overall survival rates at 1, 3, and 5 years in the hepatic resection group were 86.5%, 60.4%, and 33.3%, respectively. These rates were much higher than those in the TACE group (1-year: 77.6%; 3-year: 47.8%; and 5-year: 20.9%; P = 0.021). The long-term survival was notably better in the patients with types I and II PVTT than in the patients with types III and IV PVTT (P <0.05). The univariate and multivariate analyses indicated that types III and IV PVTT and TACE may have contributed to the poor overall survival following surgery. In HCC patients with PVTT and compensated liver function, hepatic resection is a safe and effective surgical protocol, particularly for patients with type I or II PVTT.
肝切除术在伴有门静脉癌栓(PVTT)的肝细胞癌(HCC)中的作用仍存在争议。本研究旨在评估HCC患者肝切除术与经动脉化疗栓塞术(TACE)相比的手术效果。采用回顾性研究方法,分析230例伴有门静脉侵犯的HCC患者的病历,其中96例行肝切除术,134例行TACE。比较两组患者的基线特征、肿瘤特征、临床病理参数及总生存率。肝切除术组和TACE组的基线特征和肿瘤特征具有可比性。肝切除术组的总体并发症发生率为35.4%,显著低于TACE组(73.0%,P<0.001)。然而,肝切除术组的严重并发症发生率(≥3级)为13.5%,显著高于TACE组(P = 0.003)。肝切除术组1年、3年和5年的累积总生存率分别为86.5%、60.4%和33.3%。这些生存率远高于TACE组(1年:77.6%;3年:47.8%;5年:20.9%;P = 0.021)。I型和II型PVTT患者的长期生存率明显优于III型和IV型PVTT患者(P<0.05)。单因素和多因素分析表明,III型和IV型PVTT及TACE可能是导致术后总生存率较低的原因。对于伴有PVTT且肝功能代偿的HCC患者,肝切除术是一种安全有效的手术方案,尤其适用于I型或II型PVTT患者。