Neuzillet Cindy, Babai Samy, Kempf Emmanuelle, Pujol Géraldine, Rousseau Benoît, Le-Louët Hervé
aDepartment of Medical Oncology, Henri Mondor University Hospital, Assistance Publique-Hôpitaux de Paris (AP-HP), Paris Est Créteil University (UPEC) bDepartment of Pharmacovigilance, Henri Mondor University Hospital, Assistance Publique-Hôpitaux de Paris (AP-HP), Paris Est Créteil University (UPEC) cDepartment of Pharmacology, Henri Mondor University Hospital, Assistance Publique-Hôpitaux de Paris (AP-HP), Paris Est Créteil University (UPEC), Créteil, France.
Medicine (Baltimore). 2016 Jun;95(26):e4006. doi: 10.1097/MD.0000000000004006.
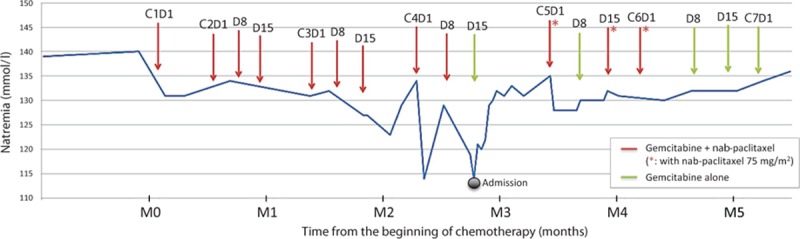
Incidence of pancreatic ductal adenocarcinoma (PDAC) is increasing. Most patients have advanced disease at diagnosis and therapeutic options in this setting are limited. Gemcitabine plus nab-paclitaxel regimen was demonstrated to increase survival compared with gemcitabine monotherapy and is therefore indicated as first-line therapy in patients with metastatic PDAC and performance status Eastern Cooperative Oncology Group (ECOG) 0-2. The safety profile of gemcitabine and nab-paclitaxel combination includes neutropenia, fatigue, and neuropathy as most common adverse events of grade 3 or higher. No case of severe hyponatremia associated with the use of nab-paclitaxel for the treatment of PDAC has been reported to date.We report the case of a 72-year-old Caucasian man with a metastatic PDAC treated with gemcitabine and nab-paclitaxel regimen, who presented with a severe hyponatremia (grade 4) caused by a documented syndrome of inappropriate antidiuretic hormone secretion (SIADH). This SIADH was attributed to nab-paclitaxel after a rigorous imputability analysis, including a rechallenge procedure with dose reduction. After dose and schedule adjustment, nab-paclitaxel was pursued without recurrence of severe hyponatremia and with maintained efficacy.Hyponatremia is a rare but potentially severe complication of nab-paclitaxel therapy that medical oncologists and gastroenterologists should be aware of. Nab-paclitaxel-induced hyponatremia is manageable upon dose and schedule adaptation, and should not contraindicate careful nab-paclitaxel reintroduction. This is of particular interest for a disease in which the therapeutic options are limited.
胰腺导管腺癌(PDAC)的发病率正在上升。大多数患者在诊断时已处于晚期疾病阶段,在此情况下的治疗选择有限。与吉西他滨单药治疗相比,吉西他滨加纳米白蛋白结合型紫杉醇方案已被证明可提高生存率,因此被指定为转移性PDAC且东部肿瘤协作组(ECOG)体能状态为0 - 2的患者的一线治疗方案。吉西他滨和纳米白蛋白结合型紫杉醇联合使用的安全性特征包括中性粒细胞减少、疲劳和神经病变,这些是最常见的3级或更高等级的不良事件。迄今为止,尚未有与使用纳米白蛋白结合型紫杉醇治疗PDAC相关的严重低钠血症病例报告。我们报告了一例72岁的白种男性转移性PDAC患者,其接受吉西他滨和纳米白蛋白结合型紫杉醇方案治疗,出现了由记录在案的抗利尿激素分泌不当综合征(SIADH)引起的严重低钠血症(4级)。经过严格的因果关系分析,包括剂量降低的再激发程序,这种SIADH归因于纳米白蛋白结合型紫杉醇。在调整剂量和给药方案后,继续使用纳米白蛋白结合型紫杉醇,未再出现严重低钠血症,且疗效维持。低钠血症是纳米白蛋白结合型紫杉醇治疗罕见但可能严重的并发症,肿瘤内科医生和胃肠病学家应予以关注。纳米白蛋白结合型紫杉醇引起的低钠血症在调整剂量和给药方案后是可控制的,不应成为谨慎重新引入纳米白蛋白结合型紫杉醇的禁忌证。对于一种治疗选择有限的疾病而言,这一点尤为重要。