Chatzipanagiotou S, Ioannidis A, Trikka-Graphakos E, Charalampaki N, Sereti C, Piccinini R, Higgins A M, Buranda T, Durvasula R, Hoogesteijn A L, Tegos G P, Rivas Ariel L
Department of Biopathology and Clinical Microbiology, Aeginition Hospital, Medical School, National and Kapodistrian University of Athens , Athens , Greece.
Department of Nursing, Faculty of Human Movement and Quality of Life Sciences, University of Peloponnese , Sparta , Greece.
Front Immunol. 2016 Jun 10;7:217. doi: 10.3389/fimmu.2016.00217. eCollection 2016.
To extract more information, the properties of infectious disease data, including hidden relationships, could be considered. Here, blood leukocyte data were explored to elucidate whether hidden information, if uncovered, could forecast mortality.
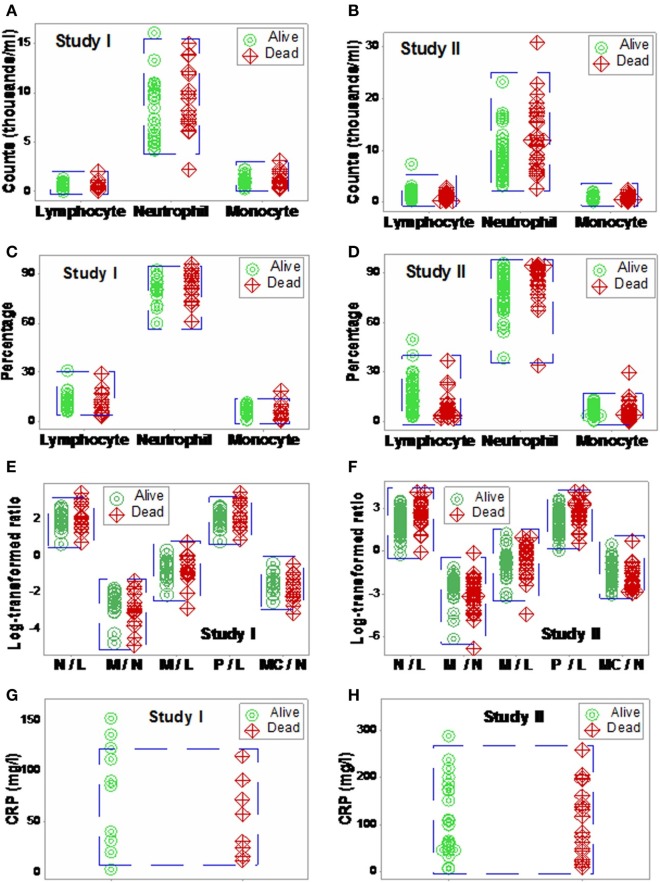
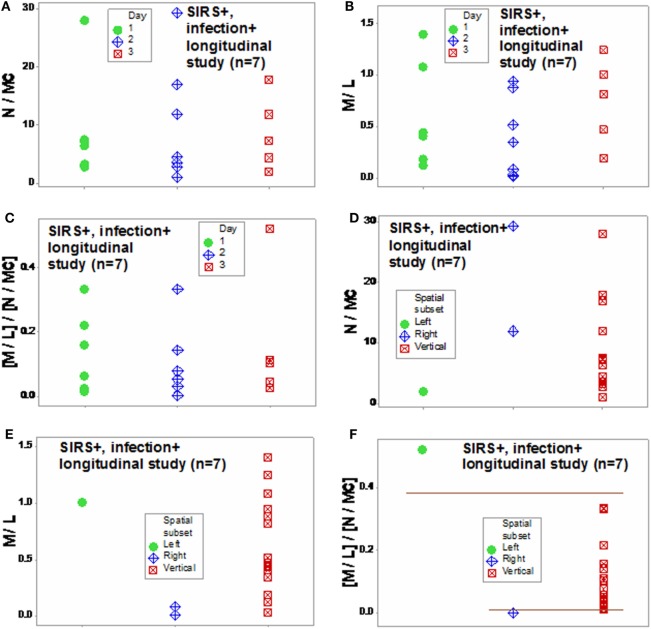
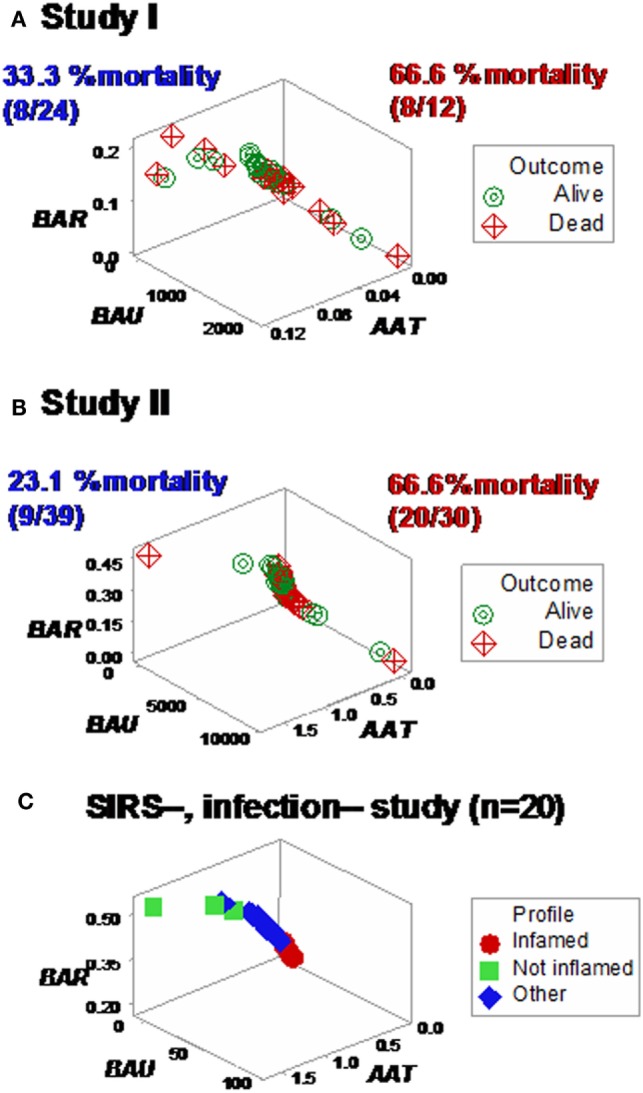
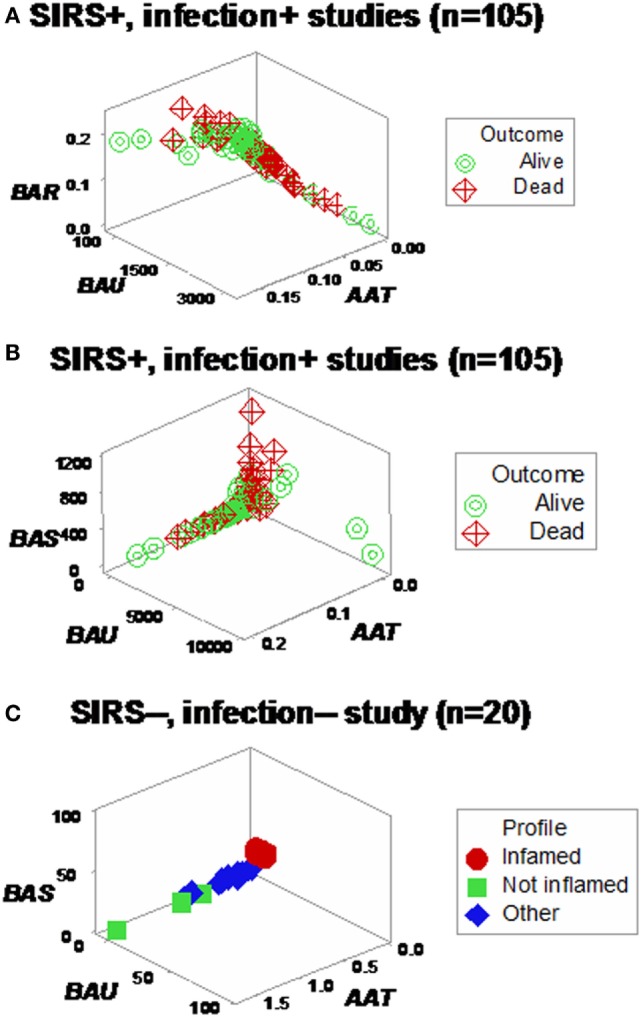
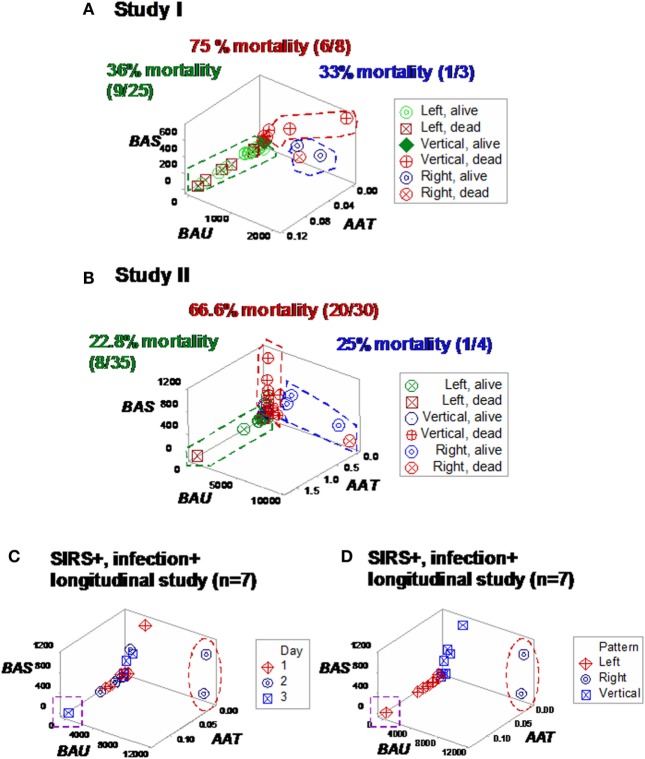
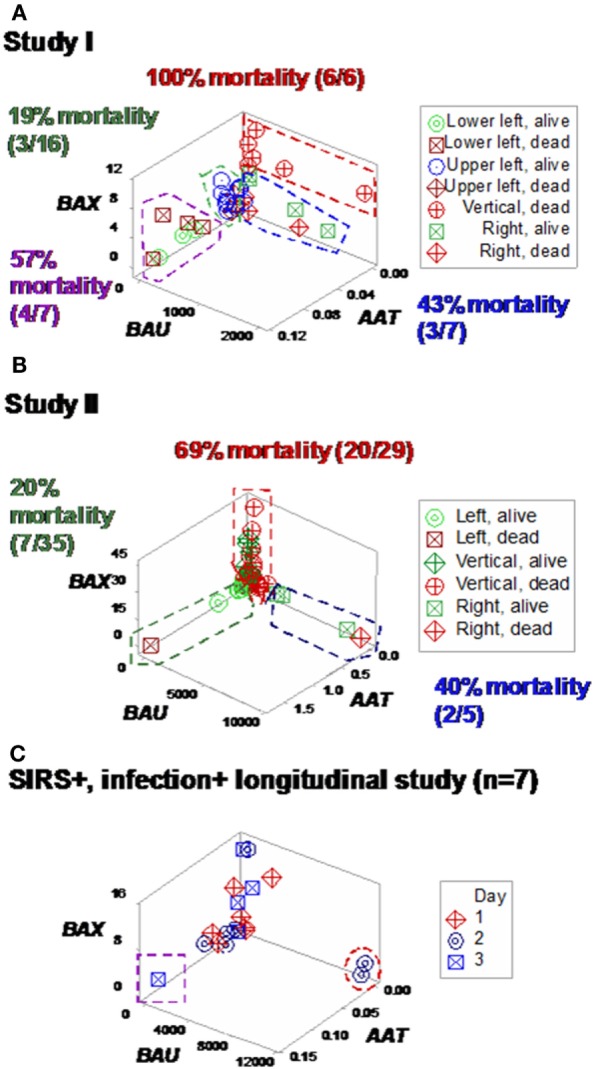
Three sets of individuals (n = 132) were investigated, from whom blood leukocyte profiles and microbial tests were conducted (i) cross-sectional analyses performed at admission (before bacteriological tests were completed) from two groups of hospital patients, randomly selected at different time periods, who met septic criteria [confirmed infection and at least three systemic inflammatory response syndrome (SIRS) criteria] but lacked chronic conditions (study I, n = 36; and study II, n = 69); (ii) a similar group, tested over 3 days (n = 7); and (iii) non-infected, SIRS-negative individuals, tested once (n = 20). The data were analyzed by (i) a method that creates complex data combinations, which, based on graphic patterns, partitions the data into subsets and (ii) an approach that does not partition the data. Admission data from SIRS+/infection+ patients were related to 30-day, in-hospital mortality.
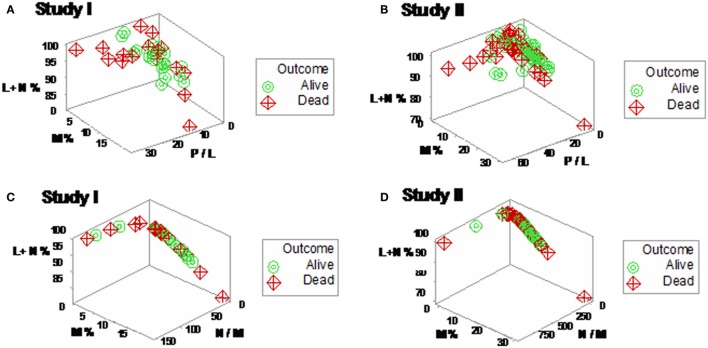
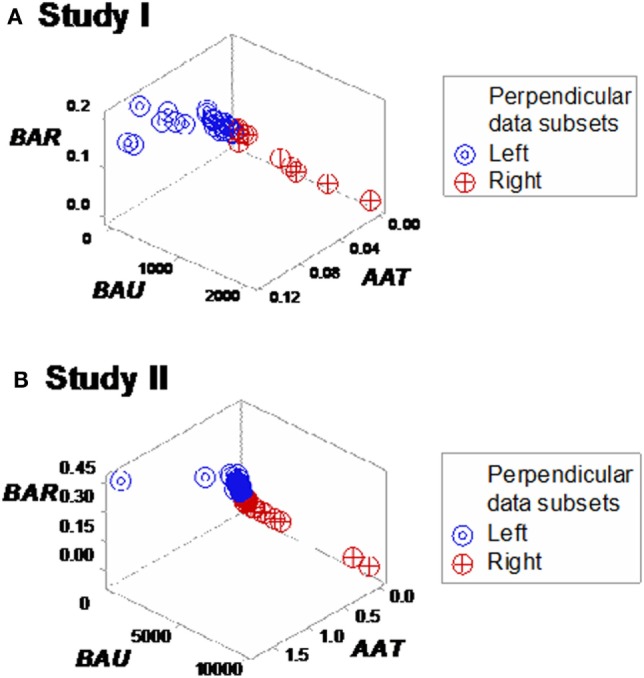
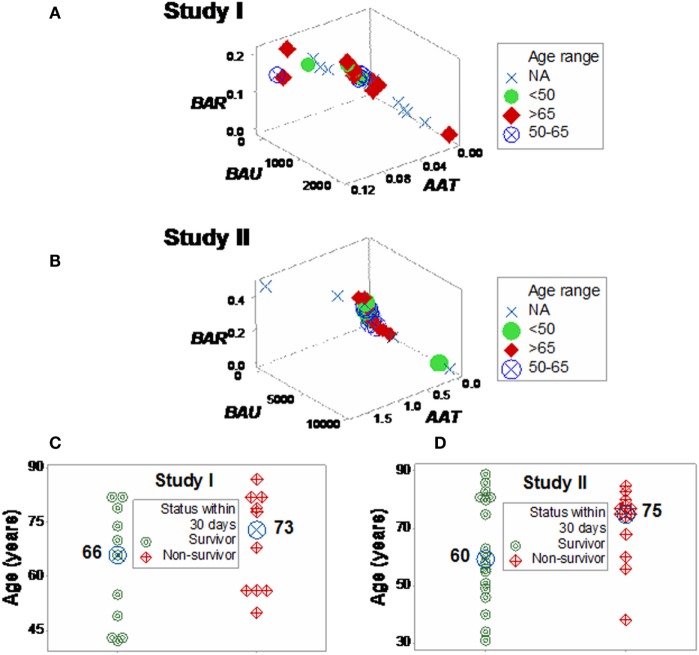
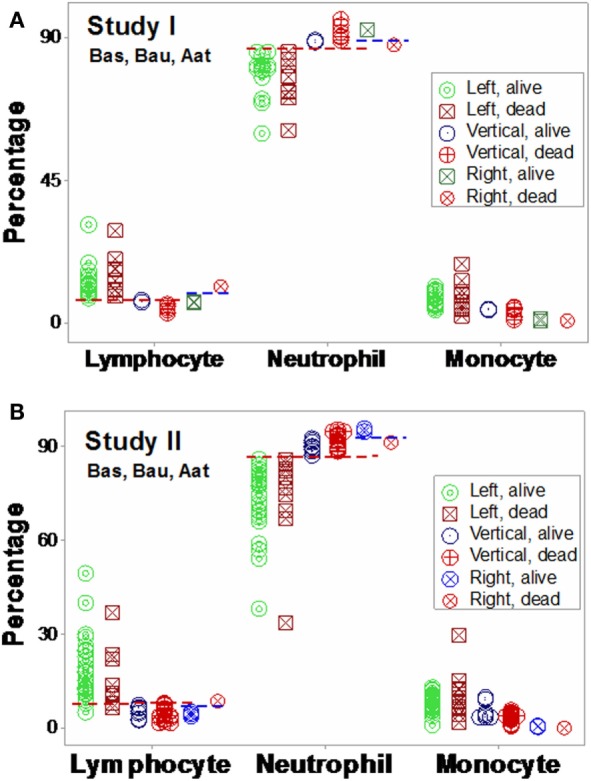
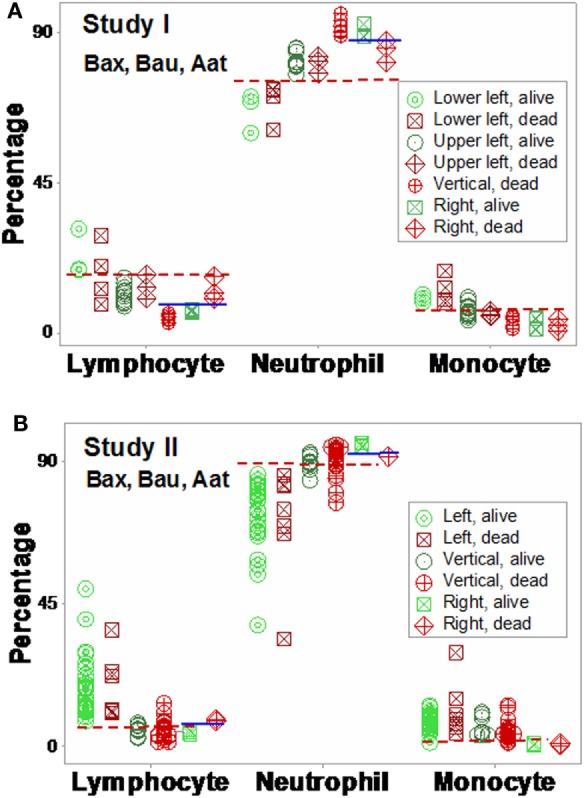
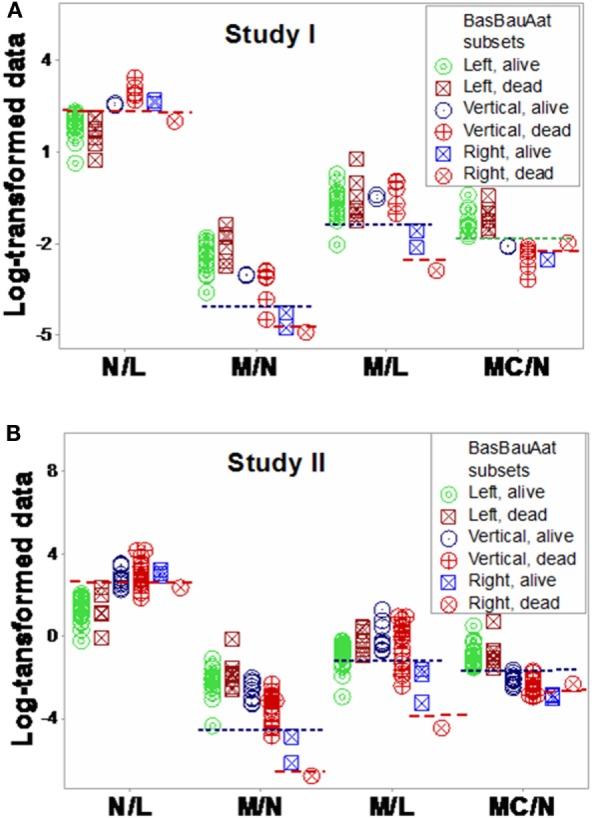
The non-partitioning approach was not informative: in both study I and study II, the leukocyte data intervals of non-survivors and survivors overlapped. In contrast, the combinatorial method distinguished two subsets that, later, showed twofold (or larger) differences in mortality. While the two subsets did not differ in gender, age, microbial species, or antimicrobial resistance, they revealed different immune profiles. Non-infected, SIRS-negative individuals did not express the high-mortality profile. Longitudinal data from septic patients displayed the pattern associated with the highest mortality within the first 24 h post-admission. Suggesting inflammation coexisted with immunosuppression, one high-mortality sub-subset displayed high neutrophil/lymphocyte ratio values and low lymphocyte percents. A second high-mortality subset showed monocyte-mediated deficiencies. Numerous within- and between-subset comparisons revealed statistically significantly different immune profiles.
While the analysis of non-partitioned data can result in information loss, complex (combinatorial) data structures can uncover hidden patterns, which guide data partitioning into subsets that differ in mortality rates and immune profiles. Such information can facilitate diagnostics, monitoring of disease dynamics, and evaluation of subset-specific, patient-specific therapies.
为了提取更多信息,可以考虑传染病数据的属性,包括隐藏关系。在此,对血液白细胞数据进行了探索,以阐明若发现隐藏信息,其是否能够预测死亡率。
对三组个体(n = 132)进行了调查,对他们进行了血液白细胞分析和微生物检测:(i)对在不同时间段随机选取的两组符合脓毒症标准(确诊感染且至少符合三项全身炎症反应综合征[SIRS]标准)但无慢性病的住院患者在入院时(细菌学检测完成前)进行横断面分析(研究I,n = 36;研究II,n = 69);(ii)对一组类似患者进行为期3天的检测(n = 7);(iii)对未感染、SIRS阴性个体进行一次检测(n = 20)。通过以下方法对数据进行分析:(i)一种创建复杂数据组合的方法,该方法基于图形模式将数据划分为子集;(ii)一种不划分数据的方法。SIRS+/感染+患者的入院数据与30天院内死亡率相关。
不划分数据的方法没有提供有用信息:在研究I和研究II中,非幸存者和幸存者的白细胞数据区间重叠。相比之下,组合方法区分出两个子集,随后这两个子集在死亡率上显示出两倍(或更大)的差异。虽然这两个子集在性别、年龄、微生物种类或抗菌药物耐药性方面没有差异,但它们显示出不同的免疫特征。未感染、SIRS阴性个体未表现出高死亡率特征。脓毒症患者的纵向数据显示,入院后24小时内呈现出与最高死亡率相关的模式。一个高死亡率子子集显示出高中性粒细胞/淋巴细胞比值和低淋巴细胞百分比,提示炎症与免疫抑制并存。第二个高死亡率子集显示单核细胞介导的缺陷。众多子集内和子集间的比较显示免疫特征存在统计学显著差异。
虽然对未划分数据的分析可能导致信息丢失,但复杂(组合)数据结构可以揭示隐藏模式,这些模式可指导将数据划分为死亡率和免疫特征不同的子集。此类信息有助于诊断、监测疾病动态以及评估针对特定子集、特定患者的治疗方法。