Omura Taku, Watanabe Eizo, Otsuka Yasufumi, Yoshida Yoko, Kato Hideki, Nangaku Masaomi, Miyata Toshiyuki, Oda Shigeto
Department of Emergency and Critical Care Medicine, Graduate School of Medicine, Chiba University, Chiba Department of Pediatrics, Faculty of Medicine, Saga University, Saga Division of Nephrology and Endocrinology, Graduate School of Medicine, The University of Tokyo, Tokyo Department of Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Osaka, Japan.
Medicine (Baltimore). 2016 Jul;95(27):e4104. doi: 10.1097/MD.0000000000004104.
To describe a case of complete remission of thrombotic microangiopathy after treatment with eculizumab in a patient with non-Shiga toxin-associated bacterial enteritis.
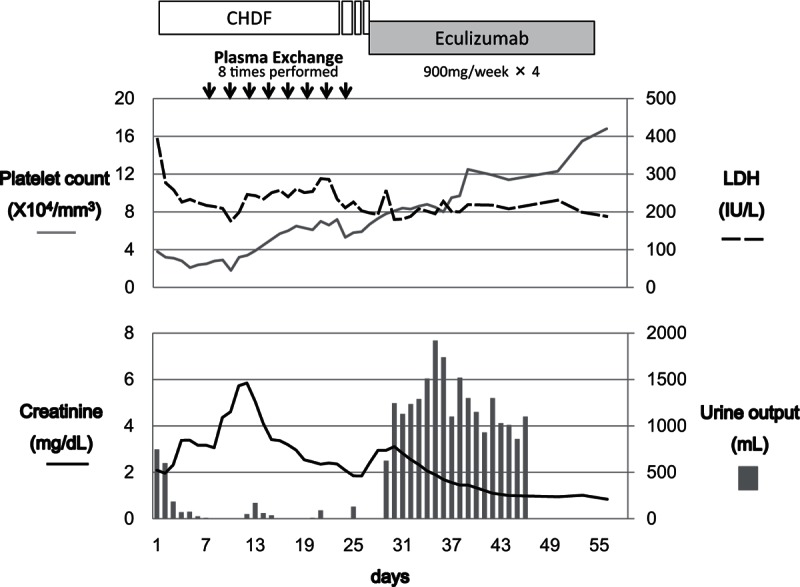
Medical/surgical intensive care unit (ICU) of a university teaching hospital.A 62-year-old man presented to a local hospital with mucous and bloody stool persisting for 1 month and worsening abdominal pain for 2 weeks. He had thrombocytopenia and renal dysfunction and was admitted with a diagnosis of sepsis due to intraabdominal infection. However, he did not respond to antimicrobial therapy, and after 7 days he was transferred to the Chiba University Hospital ICU.Antimicrobial therapy was continued, and continuous hemodiafiltration was initiated on ICU day 3, but the patient's condition deteriorated and he became anuric. Plasma exchange (PE) was initiated on ICU day 11, but anuria and thrombocytopenia persisted. Intravenous eculizumab therapy was initiated on day 26 and resulted in quick recovery of urine output and platelet count and successful discontinuation of renal support.The diagnosis of thrombotic microangiopathy was established by the presence of schistocytes on the peripheral blood smear on ICU day 9. A plasma sample collected prior to initiation of PE showed a disintegrin-like and metalloproteinase with thrombospondin type 1 motifs member 13 (ADAMTS13) activity level of >10% (25.1%). The absence of both Shiga-toxin producing E coli in feces and anti-Shiga-toxin antibody in blood led to suspicion of atypical hemolytic uremic syndrome (aHUS). Genetic test identified a nonsynonymous mutation (p.Ala311Val) in the membrane cofactor protein gene (MCP).Although the pathological significance is currently unknown, this mutation may have been the cause of adult-onset aHUS in our patient. In this case, eculizumab was successfully introduced and discontinued, and the patient remained relapse-free after 1 year of follow-up. The duration of eculizumab therapy for patients with aHUS should be determined on a case-by-case basis and possibly according to the causative genetic mutation, even though discontinuation of eculizumab therapy once initiated is not generally recommended.
描述1例非志贺毒素相关细菌性肠炎患者接受依库珠单抗治疗后血栓性微血管病完全缓解的病例。
一所大学教学医院的内科/外科重症监护病房(ICU)。一名62岁男性因黏液血便持续1个月、腹痛加重2周就诊于当地医院。他有血小板减少症和肾功能不全,因腹腔感染伴脓毒症入院。然而,他对抗菌治疗无反应,7天后转至千叶大学医院ICU。继续进行抗菌治疗,并于ICU第3天开始持续血液透析滤过,但患者病情恶化,出现无尿。ICU第11天开始进行血浆置换(PE),但无尿和血小板减少持续存在。第26天开始静脉注射依库珠单抗治疗,尿量和血小板计数迅速恢复,成功停用肾脏支持治疗。ICU第9天外周血涂片出现裂体细胞,确诊为血栓性微血管病。PE开始前采集的血浆样本显示,具有血小板反应蛋白基序的解聚素样金属蛋白酶13(ADAMTS13)活性水平>10%(25.1%)。粪便中未检出产志贺毒素大肠杆菌,血液中未检出抗志贺毒素抗体,怀疑为非典型溶血性尿毒症综合征(aHUS)。基因检测在膜辅助蛋白基因(MCP)中发现一个非同义突变(p.Ala311Val)。虽然目前尚不清楚该突变的病理意义,但可能是本例患者成人期aHUS的病因。本例中,依库珠单抗成功应用并停用后,患者随访1年无复发。对于aHUS患者,依库珠单抗治疗的持续时间应根据具体情况确定,可能还需根据致病基因突变来确定,尽管一般不建议一旦开始依库珠单抗治疗就停药。