Abe Tomohiro, Sasaki Akira, Ueda Taichiro, Miyakawa Yoshitaka, Ochiai Hidenobu
Department of Trauma and Critical Care Medicine, University of Miyazaki Hospital, Miyazaki, Japan Department of General Internal Medicine, Saitama Medical University, Saitama, Japan.
Medicine (Baltimore). 2017 Feb;96(6):e6056. doi: 10.1097/MD.0000000000006056.
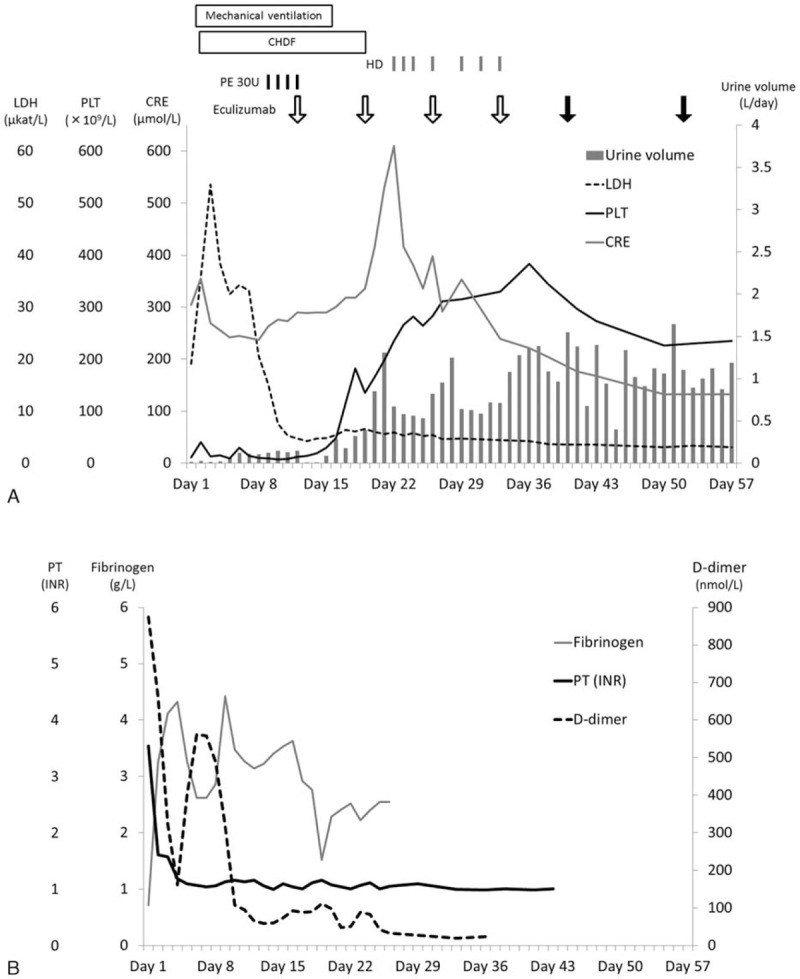
Secondary thrombotic microangiopathies (TMAs) are induced by several underlying conditions; most are resolved by treating background disease. Eculizumab is a human monoclonal antibody that blocks the final stage of the complement system and effectively treats atypical hemolytic uremic syndrome (aHUS). In this report, we present a patient with TMA secondary to sepsis- induced coagulopathy, who was successfully treated with eculizumab.A 44-year-old woman, who had no special medical history or familial history of TMAs, was admitted on suspicion of septic shock. Physical examination revealed gangrene on her soles. Blood tests revealed a decreased platelet count, disseminated intravascular coagulation (DIC), renal dysfunction, hemolysis, and infection. Although the coagulation disorder improved with intensive care, the low platelet count, elevated lactate dehydrogenase levels, and renal dysfunction persisted. Our investigations subsequently excluded thrombotic thrombocytopenic purpura and Shiga toxin-producing Escherichia coli-induced HUS. Plasma exchange only improved lactate dehydrogenase levels. We clinically diagnosed this case as atypical HUS and started eculizumab treatment. The patient's platelet count increased, her renal dysfunction improved, and the gangrene on her feet was ameliorated. The patient was discharged without maintenance dialysis therapy after approximately 3 months. Subsequent tests revealed elevated serum levels of soluble C5b-9, and genetic testing revealed compound heterozygous c.184G > A (Val62Ile) and c.1204T > C (Tyr402His) single-nucleotide polymorphisms in complement factor H.We encountered a case of complement-mediated TMA accompanied by DIC, which was successfully treated with eculizumab. Further studies are necessary to support the optimal use of eculizumab for TMA with background diseases.
继发性血栓性微血管病(TMA)由多种潜在疾病诱发;多数可通过治疗基础疾病得到缓解。依库珠单抗是一种人源单克隆抗体,可阻断补体系统的终末阶段,有效治疗非典型溶血性尿毒症综合征(aHUS)。在本报告中,我们介绍了一名继发于脓毒症诱导凝血病的TMA患者,该患者接受依库珠单抗治疗成功。一名44岁女性,无特殊病史或TMA家族史,因疑似感染性休克入院。体格检查发现其足底有坏疽。血液检查显示血小板计数降低、弥散性血管内凝血(DIC)、肾功能不全、溶血及感染。尽管通过重症监护凝血障碍有所改善,但血小板计数低、乳酸脱氢酶水平升高及肾功能不全仍持续存在。我们的检查随后排除了血栓性血小板减少性紫癜和产志贺毒素大肠杆菌诱导的HUS。血浆置换仅改善了乳酸脱氢酶水平。我们临床诊断该病例为非典型HUS并开始依库珠单抗治疗。患者的血小板计数增加,肾功能改善,足部坏疽减轻。约3个月后患者未接受维持性透析治疗而出院。随后的检查显示可溶性C5b - 9血清水平升高,基因检测显示补体因子H存在复合杂合性c.184G>A(Val62Ile)和c.1204T>C(Tyr402His)单核苷酸多态性。我们遇到一例伴有DIC的补体介导的TMA病例,该病例接受依库珠单抗治疗成功。需要进一步研究以支持依库珠单抗在伴有基础疾病的TMA中的最佳应用。