Paul Subroto, Lee Paul C, Mao Jialin, Isaacs Abby J, Sedrakyan Art
Department of Cardiothoracic Surgery, RWJ Barnabas Health System, West Orange, NJ, USA.
Department of Thoracic Surgery, New York Presbyterian Hospital/Queens, NY, USA.
BMJ. 2016 Jul 8;354:i3570. doi: 10.1136/bmj.i3570.
To compare cancer specific survival after thoracoscopic sublobar lung resection and stereotactic ablative radiotherapy (SABR) for tumors ≤2 cm in size and thoracoscopic resection (sublobar resection or lobectomy) and SABR for tumors ≤5 cm in size.
National population based retrospective cohort study with propensity matched comparative analysis.
Surveillance, Epidemiology, and End Results (SEER) registry linked with Medicare database in the United States.
Patients aged ≥66 with lung cancer undergoing SABR or thoracoscopic lobectomy or sublobar resection from 1 Oct 2007 to 31 June 2012 and followed up to 31 December 2013.
Cancer specific survival after SABR or thoracoscopic surgery for lung cancer.
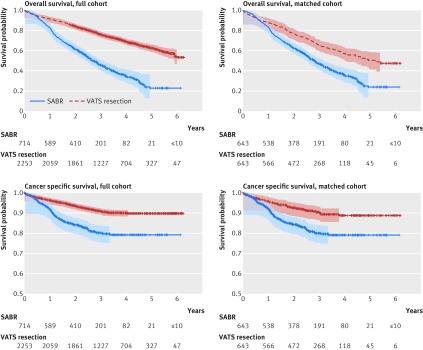
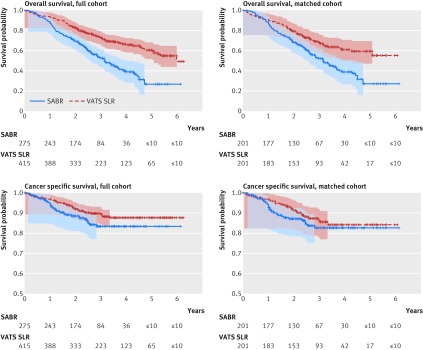
690 (275 (39.9%) SABR and 415 (60.1%) thoracoscopic sublobar lung resection) and 2967 (714 (24.1%) SABR and 2253 (75.9%) thoracoscopic resection) patients were included in primary and secondary analyses. The average age of the entire cohort was 76. Follow-up of the entire cohort ranged from 0 to 6.25 years, with an average of three years. In the primary analysis of patients with tumors sized ≤2 cm, 37 (13.5%) undergoing SABR and 44 (10.6%) undergoing thoracoscopic sublobar resection died from lung cancer, respectively. The cancer specific survival diverged after one year, but in the matched analysis (201 matched patients in each group) there was no significant difference between the groups (SABR v sublobar lung resection mortality: hazard ratio 1.32, 95% confidence interval 0.77 to 2.26; P=0.32). Estimated cancer specific survival at three years after SABR and thoracoscopic sublobar lung resection was 82.6% and 86.4%, respectively. The secondary analysis (643 matched patients in each group) showed that thoracoscopic resection was associated with improved cancer specific survival over SABR in patients with tumors sized ≤5 cm (SABR v resection mortality: hazard ratio 2.10, 1.52 to 2.89; P<0.001). Estimated cancer specific survival at three years was 80.0% and 90.3%, respectively.
This propensity matched analysis suggests that patients undergoing thoracoscopic surgical resection, particularly for larger tumors, might have improved cancer specific survival compared with patients undergoing SABR. Despite strategies used in study design and propensity matching analysis, there are inherent limitations to this observational analysis related to confounding, similar to most studies in healthcare of non-surgical technologies compared with surgery. As the adoption of SABR for the treatment of early stage operable lung cancer would be a paradigm shift in lung cancer care, it warrants further thorough evaluation before widespread adoption in practice.
比较胸腔镜肺叶下切除与立体定向消融放疗(SABR)治疗直径≤2 cm肿瘤以及胸腔镜切除(肺叶下切除或肺叶切除)与SABR治疗直径≤5 cm肿瘤后的癌症特异性生存率。
基于全国人群的回顾性队列研究,并进行倾向匹配比较分析。
美国监测、流行病学和最终结果(SEER)登记处与医疗保险数据库相链接。
2007年10月1日至2012年6月31日期间接受SABR或胸腔镜肺叶切除或肺叶下切除的≥66岁肺癌患者,随访至2013年12月31日。
肺癌患者接受SABR或胸腔镜手术后的癌症特异性生存率。
690例(275例(39.9%)接受SABR,415例(60.1%)接受胸腔镜肺叶下切除)和2967例(714例(24.1%)接受SABR,2253例(75.9%)接受胸腔镜切除)患者分别纳入了一级和二级分析。整个队列的平均年龄为76岁。整个队列的随访时间为0至6.25年,平均为3年。在对直径≤2 cm肿瘤患者的一级分析中,分别有37例(13.5%)接受SABR和44例(10.6%)接受胸腔镜肺叶下切除的患者死于肺癌。癌症特异性生存率在1年后出现差异,但在匹配分析中(每组201例匹配患者)两组之间无显著差异(SABR与肺叶下切除死亡率:风险比1.32,95%置信区间0.77至2.26;P = 0.32)。SABR和胸腔镜肺叶下切除后3年的估计癌症特异性生存率分别为82.6%和86.4%。二级分析(每组643例匹配患者)显示,对于直径≤5 cm的肿瘤患者,胸腔镜切除与SABR相比,癌症特异性生存率有所提高(SABR与切除死亡率:风险比2.10,1.52至2.89;P<0.001)。3年的估计癌症特异性生存率分别为80.0%和90.3%。
这项倾向匹配分析表明,与接受SABR的患者相比,接受胸腔镜手术切除的患者,尤其是对于较大肿瘤的患者,癌症特异性生存率可能有所提高。尽管在研究设计和倾向匹配分析中采用了一些策略,但与大多数非手术技术与手术在医疗保健方面的研究类似,这种观察性分析存在与混杂因素相关的固有局限性。由于采用SABR治疗早期可手术肺癌将是肺癌治疗模式的转变,在实际广泛应用之前,有必要进行进一步深入评估。