Frangieh Antonio H, Obeid Slayman, Ghadri Jelena-Rima, Imori Yoichi, D'Ascenzo Fabrizio, Kovac Marc, Ruschitzka Frank, Lüscher Thomas F, Duru Firat, Templin Christian
Department of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerland.
Department of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerland
J Am Heart Assoc. 2016 Jun 13;5(6):e003418. doi: 10.1161/JAHA.116.003418.
ECG criteria differentiating Takotsubo cardiomyopathy (TTC) from mainly anterior myocardial infarction (MI) have been suggested; however, this was in small patient populations.
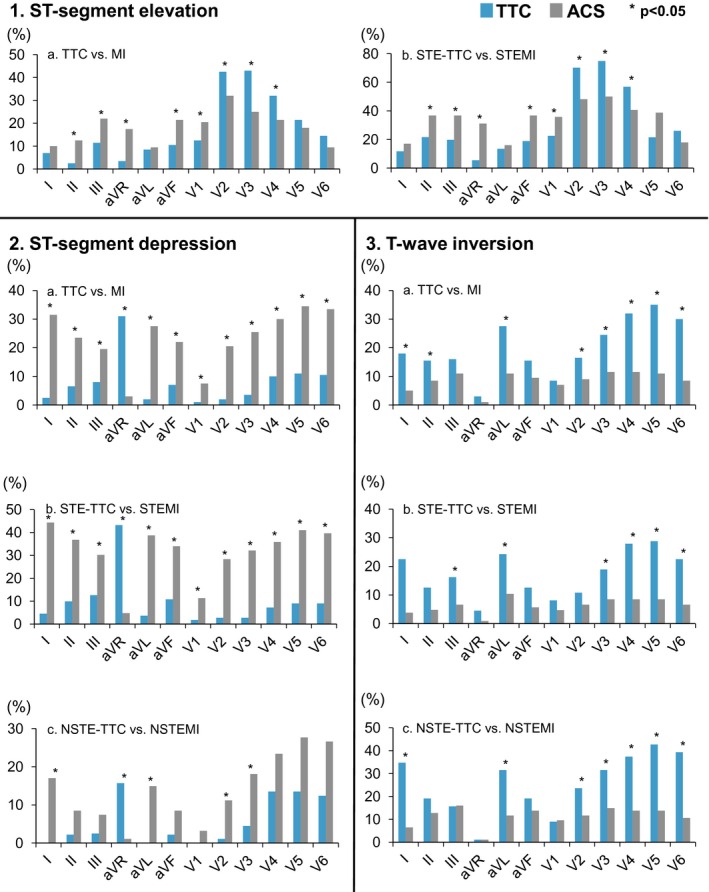
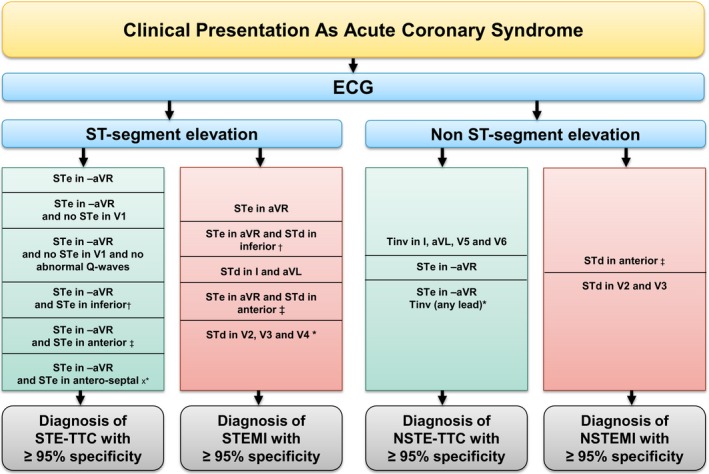
Twelve-lead admission ECGs of consecutive 200 TTC and 200 MI patients were compared in dichotomized groups based on the presence or absence of ST-elevation MI (STEMI versus STE-TTC and non-ST elevation MI versus non ST-elevation-TTC). When comparing STEMI and STE-TTC, ST-elevation in -aVR was characteristic of STE-TTC with a sensitivity/specificity of 43% and 95%, positive predictive value (PPV) 91%, and a negative predictive value (NPV) 62% (P<0.001); when ST-elevation in -aVR is accompanied by ST-elevation in inferior leads, sensitivity/specificity were 14% and 98% (PPV was 89% and NPV 52%) (P=0.001), and 12% and 100% when associated with ST-elevation in anteroseptal leads (PPV 100%, NPV 52%) (P<0.001). On the other hand, STEMI was characterized by ST-elevation in aVR (sensitivity/specificity of 31% and 95% P<0.001, PPV 85% and NPV 59%) and ST-depression in V2-V3-V4 (sensitivity/specificity of 24% and 100% P<0.001, PPV 100% and NPV 76%). When comparing non-ST elevation MI and non ST-elevation-TTC, T-inversion in leads I-aVL-V5-V6 had a sensitivity/specificity of 17% and 97% for non ST-elevation-TTC (PPV 83% and NPV 55%) (P<0.001), and ST-elevation in -aVR with T-inversion in any lead was also specific for non ST-elevation-TTC (sensitivity/specificity of 8% and 100%, PPV 100% and NPV 53%) (P=0.006). In non-ST elevation MI patients, the presence of ST-depression in V2-V3 was specific (sensitivity/specificity of 11% and 99%, PPV 91% and NPV 51%) (P=0.01).
ECG on admission can differentiate between TTC and acute MI, with high specificity and positive predictive value.
URL: https://www.clinicaltrials.gov/. Unique identifier: NCT01947621.
已有研究提出用于鉴别应激性心肌病(TTC)与主要为前壁心肌梗死(MI)的心电图标准;然而,这些研究的患者样本量较小。
将连续纳入的200例TTC患者和200例MI患者的12导联入院心电图,根据是否存在ST段抬高型心肌梗死(STEMI与ST段抬高型TTC、非ST段抬高型心肌梗死与非ST段抬高型TTC)分为两组进行比较。比较STEMI和ST段抬高型TTC时,aVR导联ST段抬高是ST段抬高型TTC的特征性表现,敏感性/特异性分别为43%和95%,阳性预测值(PPV)为91%,阴性预测值(NPV)为62%(P<0.001);当aVR导联ST段抬高伴有下壁导联ST段抬高时,敏感性/特异性分别为14%和98%(PPV为89%,NPV为52%)(P=0.001),与前间隔导联ST段抬高相关时,敏感性/特异性分别为12%和100%(PPV为100%,NPV为52%)(P<0.001)。另一方面,STEMI的特征为aVR导联ST段抬高(敏感性/特异性分别为31%和95%,P<0.001,PPV为85%,NPV为59%)以及V2-V3-V4导联ST段压低(敏感性/特异性分别为24%和100%,P<0.001,PPV为100%,NPV为76%)。比较非ST段抬高型心肌梗死和非ST段抬高型TTC时,I-aVL-V5-V6导联T波倒置对非ST段抬高型TTC的敏感性/特异性分别为17%和97%(PPV为83%,NPV为55%)(P<0.001),aVR导联ST段抬高伴任何导联T波倒置对非ST段抬高型TTC也具有特异性(敏感性/特异性分别为8%和100%,PPV为100%,NPV为53%)(P=0.006)。在非ST段抬高型心肌梗死患者中,V2-V3导联ST段压低具有特异性(敏感性/特异性分别为11%和99%,PPV为91%,NPV为51%)(P=0.01)。
入院时的心电图能够以高特异性和阳性预测值鉴别TTC与急性心肌梗死。