Gharzai Laila, Verma Vivek, Denniston Kyle A, Bhirud Abhijeet R, Bennion Nathan R, Lin Chi
College of Medicine, University of Nebraska Medical Center, Omaha, NE, United States of America.
Department of Radiation Oncology, University of Nebraska Medical Center, Omaha, NE, United States of America.
PLoS One. 2016 Jul 18;11(7):e0158916. doi: 10.1371/journal.pone.0158916. eCollection 2016.
Radiation therapy (RT) for esophageal cancer often results in unintended radiation doses delivered to the heart owing to anatomic proximity. Using the Surveillance, Epidemiology, and End Results (SEER) database, we examined late cardiac death in survivors of esophageal cancer that had or had not received RT.
5,630 patients were identified that were diagnosed with esophageal squamous cell carcinoma (SCC) or adenocarcinoma (AC) from 1973-2012, who were followed for at least 5 years after therapy. Examined risk factors for cardiac death included age (≤55/56-65/66-75/>75), gender, race (white/non-white), stage (local/regional/distant), histology (SCC/AC), esophageal location (<18cm/18-24cm/25-32cm/33-40cm from incisors), diagnosis year (1973-1992/1993-2002/2003-2012), and receipt of surgery and/or RT. Time to cardiac death was evaluated using the Kaplan-Meier method. A Cox model was used to evaluate risk factors for cardiac death in propensity score matched data.
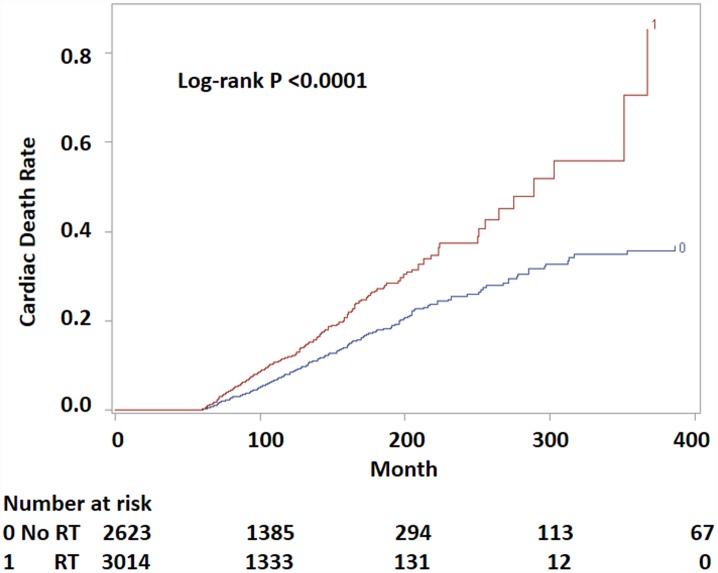
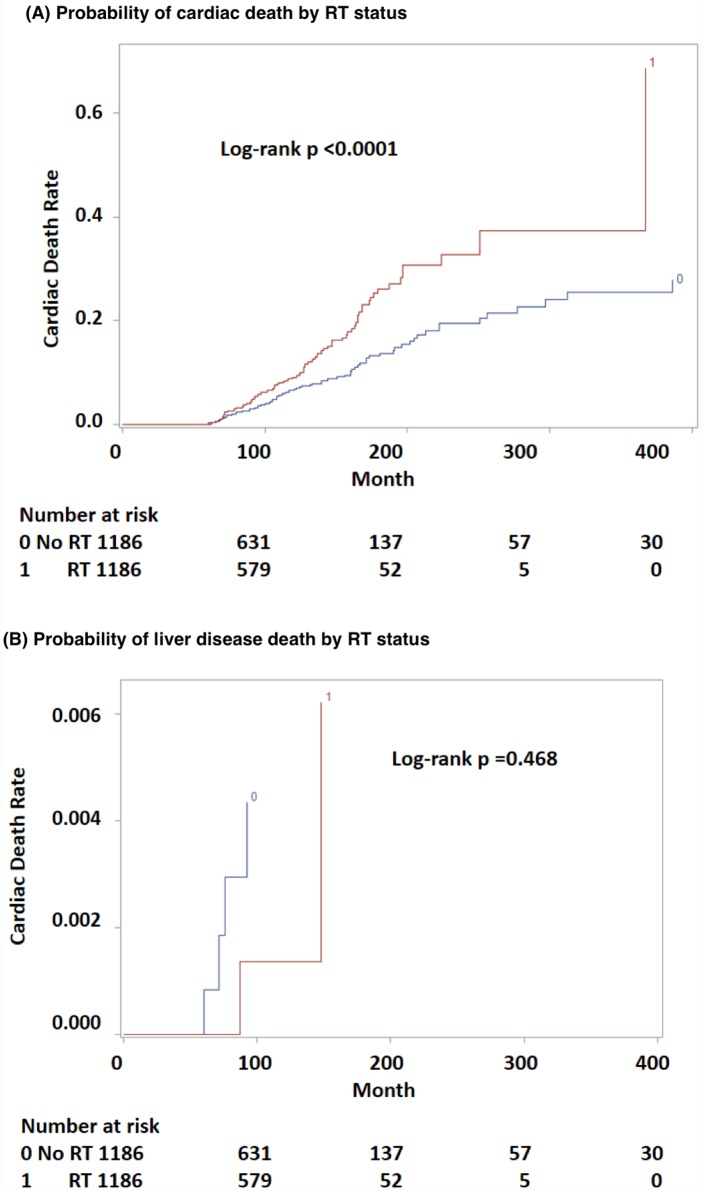
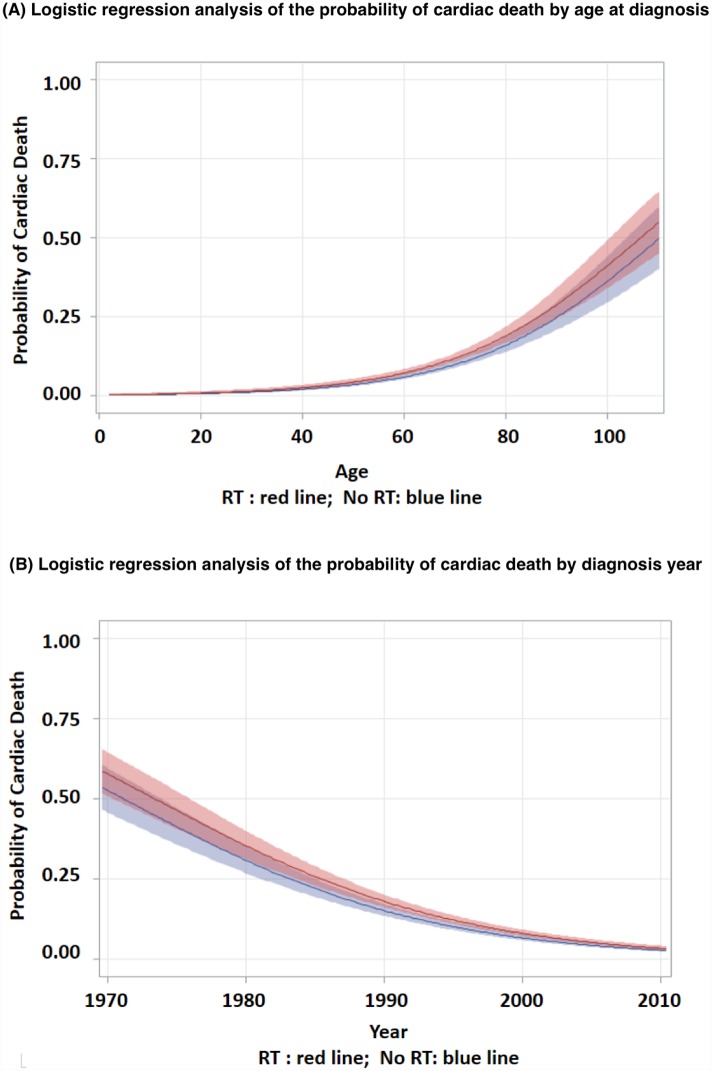
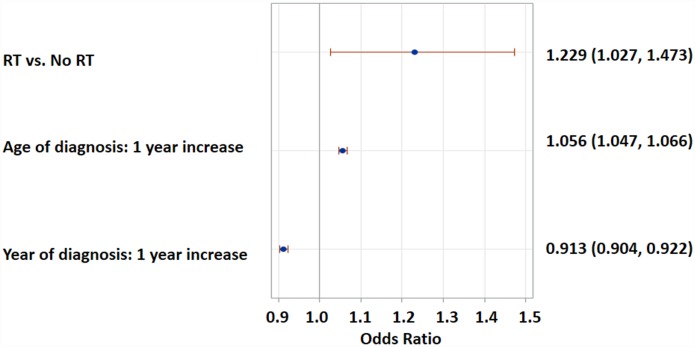
Patients who received RT were younger, diagnosed more recently, had more advanced disease, SCC histology, and no surgery. The RT group had higher risk of cardiac death than the no-RT group (log-rank p<0.0001). The median time to cardiac death in the RT group was 289 months (95% CI, 255-367) and was not reached in the no-RT group. The probability of cardiac death increased with age and decreased with diagnosis year, and this trend was more pronounced in the RT group. Multivariate analysis found RT to be associated with higher probability of cardiac death (OR 1.23, 95% CI 1.03-1.47, HR 1.961, 95% CI 1.466-2.624). Lower esophageal subsite (33-40 cm) was also associated with a higher risk of cardiac death. Other variables were not associated with cardiac death.
Recognizing the limitations of a SEER analysis including lack of comorbidity accountability, these data should prompt more definitive study as to whether a possible associative effect of RT on cardiac death could potentially be a causative effect.
由于解剖位置相邻,食管癌的放射治疗(RT)常常导致心脏受到意外的辐射剂量。我们利用监测、流行病学和最终结果(SEER)数据库,研究了接受或未接受RT的食管癌幸存者的晚期心脏死亡情况。
确定了5630例在1973年至2012年期间被诊断为食管鳞状细胞癌(SCC)或腺癌(AC)的患者,这些患者在治疗后至少随访了5年。研究的心脏死亡风险因素包括年龄(≤55/56 - 65/66 - 75/>75)、性别、种族(白人/非白人)、分期(局部/区域/远处)、组织学类型(SCC/AC)、食管位置(距切牙<18cm/18 - 24cm/25 - 32cm/33 - 40cm)、诊断年份(1973 - 1992/1993 - 2002/2003 - 2012)以及是否接受手术和/或RT。使用Kaplan - Meier方法评估心脏死亡时间。在倾向评分匹配的数据中,使用Cox模型评估心脏死亡的风险因素。
接受RT的患者更年轻,诊断时间更近,疾病更晚期,组织学类型为SCC,且未接受手术。RT组心脏死亡风险高于未接受RT组(对数秩检验p<0.0001)。RT组心脏死亡的中位时间为289个月(95%可信区间,255 - 367),未接受RT组未达到该时间。心脏死亡概率随年龄增加而升高,随诊断年份降低,且这种趋势在RT组更明显。多因素分析发现RT与心脏死亡概率较高相关(比值比1.23,95%可信区间1.03 - 1.47,风险比1.961,95%可信区间1.466 - 2.624)。食管下段(33 - 40 cm)也与心脏死亡风险较高相关。其他变量与心脏死亡无关。
认识到SEER分析的局限性,包括缺乏合并症的考量,这些数据应促使开展更具确定性的研究,以确定RT对心脏死亡可能的关联效应是否可能是因果效应。