Zaydfudim Victor M, Vachharajani Neeta, Klintmalm Goran B, Jarnagin William R, Hemming Alan W, Doyle Maria B Majella, Cavaness Keith M, Chapman William C, Nagorney David M
*Division of Surgical Oncology, Section of Hepatobiliary and Pancreatic Surgery, University of Virginia, Charlottesville, VA †Department of Surgery, Section of Abdominal Transplantation, Washington University School of Medicine, St. Louis, MO ‡Annette C. and Harold C. Simmons Transplant Institute, Baylor University Medical Center, Dallas, TX §Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY ||Division of Transplantation and Hepatobiliary Surgery, University of California San Diego, San Diego, CA ¶Department of Surgery, Section of Hepatobiliary and Pancreas Surgery, Mayo Clinic College of Medicine, Rochester, MN.
Ann Surg. 2016 Oct;264(4):650-8. doi: 10.1097/SLA.0000000000001866.
To assess survival after liver resection and transplantation in patients with hepatocellular carcinoma (HCC) beyond Milan criteria.
The role of liver resection and transplantation remains controversial for patients with HCC beyond Milan criteria. Resection of advanced tumors and transplantation using extended-criteria are pursued at select high-volume center.
Patients from 5 liver cancer centers in the United States who had liver resection or transplantation for HCC beyond Milan criteria between 1990 and 2011 were included in the study. Multivariable and propensity-matching analyses estimated the effects of clinical factors and operative selection on survival.
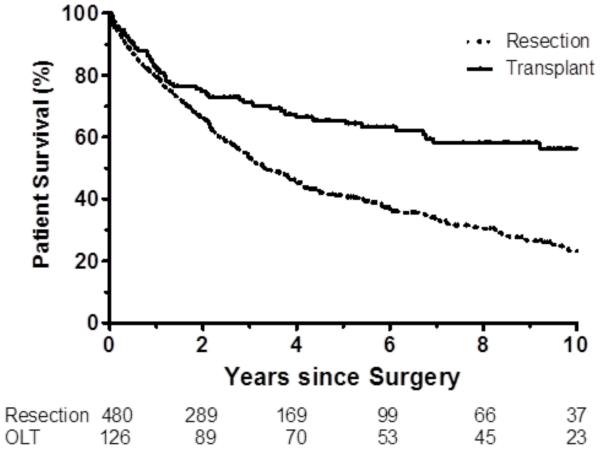
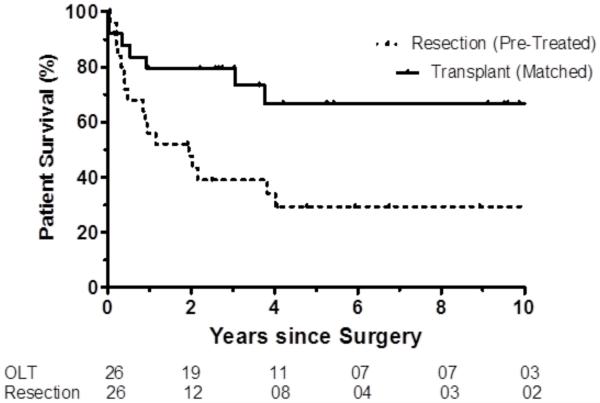
Of 608 patients beyond Milan without vascular invasion, 480 (79%) patients underwent resection and 128 (21%) underwent transplantation. Clinicopathologic profiles between resection and transplant patients differed significantly. Hepatitis C and cirrhosis were more prevalent in transplantation group (P < 0.001). Resection patients had larger tumors [median 9 cm, interquartile range (IQR): 6.5-12.9 cm vs. median 4.1, IQR: 3.4-5.3 cm, P < 0.001]; transplant patients were more likely to have multiple tumors (78% vs 28%, P < 0.001).Overall (OS) and disease-free survival (DFS) were both greater after tumor downstaging and transplantation than resection (all P < 0.001). OS did not differ between liver transplant recipients who were not pretreated or pretreated and failed to downstage compared with propensity-matched liver resection patients (P ≥ 0.176); DFS in this propensity matched cohort was greater after liver transplantation (P ≤ 0.017).
Liver resection and transplantation provide curative options for patients with HCC beyond Milan criteria. Further treatment strategies aimed at the efficiency and durability of tumor downstaging and expansion of the role of transplantation among suitable candidates could improve outcomes in patients with large or multifocal HCC.
评估超出米兰标准的肝细胞癌(HCC)患者肝切除和肝移植后的生存率。
对于超出米兰标准的HCC患者,肝切除和肝移植的作用仍存在争议。在一些高容量中心,会对晚期肿瘤进行切除,并采用扩大标准进行移植。
纳入1990年至2011年间来自美国5个肝癌中心、因超出米兰标准的HCC接受肝切除或肝移植的患者。多变量和倾向匹配分析估计了临床因素和手术选择对生存率的影响。
在608例无血管侵犯且超出米兰标准的患者中,480例(79%)接受了肝切除,128例(21%)接受了肝移植。肝切除患者和肝移植患者的临床病理特征存在显著差异。丙型肝炎和肝硬化在肝移植组更为普遍(P<0.001)。肝切除患者的肿瘤更大[中位数9cm,四分位间距(IQR):6.5 - 12.9cm,而肝移植患者中位数为4.1cm,IQR:3.4 - 5.3cm,P<0.001];肝移植患者更易出现多发肿瘤(78%对28%,P<0.001)。总体生存(OS)和无病生存(DFS)在肿瘤降期和肝移植后均高于肝切除(所有P<0.001)。与倾向匹配的肝切除患者相比,未接受预处理或接受预处理但未实现降期的肝移植受者的OS无差异(P≥0.176);在这个倾向匹配队列中,肝移植后的DFS更高(P≤0.017)。
肝切除和肝移植为超出米兰标准的HCC患者提供了治愈选择。针对肿瘤降期的效率和持久性以及在合适候选者中扩大移植作用的进一步治疗策略,可能会改善大肝癌或多灶性HCC患者的预后。