Wollersheim Tobias, Engelhardt Lilian Jo, Pachulla Jeanne, Moergeli Rudolf, Koch Susanne, Spies Claudia, Hiesmayr Michael, Weber-Carstens Steffen
Department of Anesthesiology and Operative Intensive Care Medicine, Campus Charité Mitte and Campus Virchow Klinikum, Charité - Universitätsmedizin Berlin, Augustenburger Platz 1, 13353, Berlin, Germany.
Berlin Institute of Health (BIH), Berlin, Germany.
Ann Intensive Care. 2016 Dec;6(1):70. doi: 10.1186/s13613-016-0167-z. Epub 2016 Jul 21.
Continuous glucose monitoring (CGM) has not yet been implemented in the intensive care unit (ICU) setting. The purpose of this study was to evaluate reliability, feasibility, nurse acceptance and accuracy of the Medtronic Sentrino(®) CGM system in critically ill patients.
Sensors were inserted into the subcutaneous tissue of the patient's thigh, quantifying interstitial glucose concentration for up to 72 h per sensor. Reliability and feasibility analysis included frequency of data display, data gaps and reasons for sensor removal. We surveyed nurse acceptance in a questionnaire. For the accuracy analysis, we compared sensor values to glucose values obtained via blood gas analysis. Potential benefits of CGM were investigated in intra-individual analyses of factors, such as glycemic variability or time in target range achieved with CGM compared to that achieved with intermittent glucose monitoring.
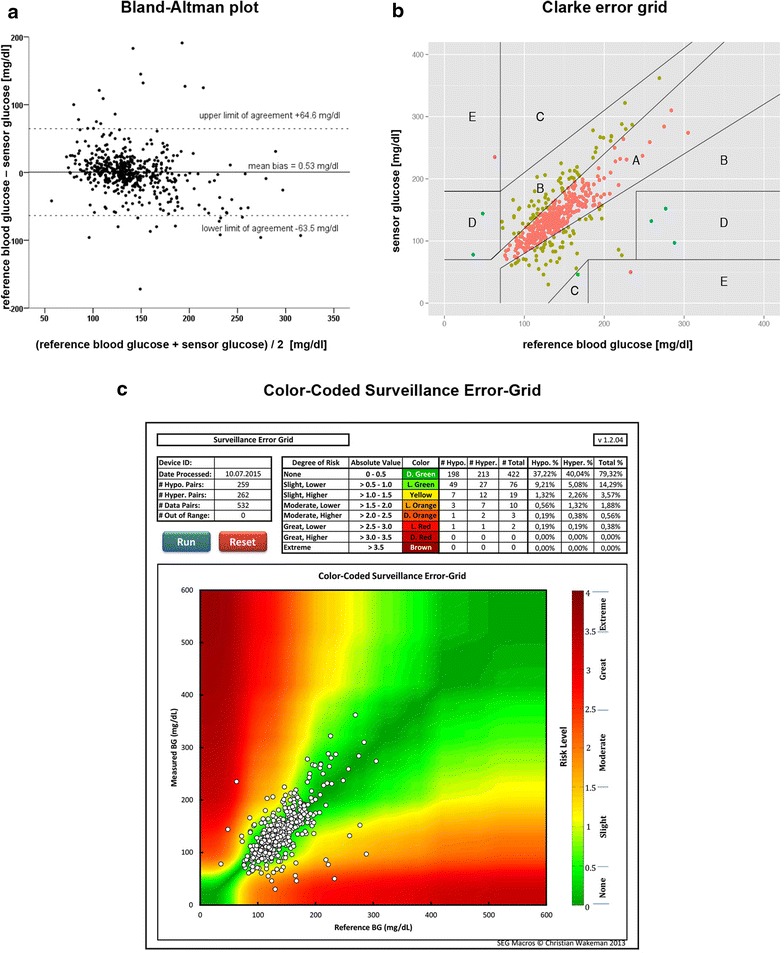
The device generated 68,655 real-time values from 31 sensors in 20 critically ill patients. 532 comparative blood glucose values were collected. Data were displayed during 32.5 h [16.0/62.4] per sensor, which is 45.1 % of the expected time of 72 h and 84.8 % of 37.9 h actual monitoring time. 21 out of 31 sensors were removed prematurely. 79.1 % of the nursing staff rated the device as not beneficial; the response rate was one-third. Mean absolute relative difference was 15.3 % (CI 13.5-17.0 %). Clarke error grid: 76.9 % zone A, 21.6 % zone B, 0.2 % zone C, 0.9 % zone D, 0.4 % zone E. Bland-Altman plot: mean bias +0.53 mg/dl, limits of agreement +64.6 and -63.5 mg/dl. Accuracy deteriorated during elevated glycemic variability and in the hyperglycemic range. There was no reduction in dysglycemic events during CGM compared to 72 h before and after CGM. If CGM was measuring accurately, it identified more hyperglycemic events when compared to intermittent measurements. This study was not designed to evaluate potential benefits of CGM on glucose control.
The subcutaneous CGM system did not perform with satisfactory accuracy, feasibility, or nursing acceptance when evaluated in 20 medical-surgical ICU patients. Low point accuracy and prolonged data gaps significantly limited the potential clinical usefulness of the CGM trend data. Accurate continuous data display, with a MARD < 14 %, showed potential benefits in a subgroup of our patients. Trial registration NCT02296372; Ethic vote Charité EA2/095/14.
连续血糖监测(CGM)尚未在重症监护病房(ICU)环境中实施。本研究的目的是评估美敦力Sentrino®CGM系统在危重症患者中的可靠性、可行性、护士接受度及准确性。
将传感器插入患者大腿的皮下组织,每个传感器最多可连续72小时定量测定组织间液葡萄糖浓度。可靠性和可行性分析包括数据显示频率、数据缺失情况及传感器移除原因。我们通过问卷调查了解护士的接受度。在准确性分析中,我们将传感器测得的值与通过血气分析获得的血糖值进行比较。通过个体内因素分析,研究CGM的潜在益处,例如与间歇性血糖监测相比,CGM的血糖变异性或达标时间。
该设备从20例危重症患者的31个传感器中生成了68,655个实时值。收集了532个对比血糖值。每个传感器的数据显示时间为32.5小时[16.0/62.4],占预期72小时的45.1%,占实际监测时间37.9小时的84.8%。31个传感器中有21个被过早移除。79.1%的护理人员认为该设备无益处;问卷回复率为三分之一。平均绝对相对差异为15.3%(95%CI 13.5 - 17.0%)。克拉克误差网格分析结果:A区76.9%,B区21.6%,C区0.2%,D区0.9%,E区0.4%。Bland - Altman图分析结果:平均偏差 +0.53mg/dl,一致性界限为 +64.6和 -63.5mg/dl。在血糖变异性增加和高血糖范围内,准确性下降。与CGM前后72小时相比,CGM期间血糖异常事件没有减少。如果CGM测量准确,与间歇性测量相比,它能识别出更多的高血糖事件。本研究并非旨在评估CGM对血糖控制的潜在益处。
在20例内科 - 外科ICU患者中进行评估时,皮下CGM系统在准确性、可行性或护士接受度方面表现不佳。低点准确性和长时间的数据缺失显著限制了CGM趋势数据的潜在临床实用性。在我们的部分患者亚组中,准确的连续数据显示(平均绝对相对差异<14%)显示出潜在益处。试验注册号NCT02296372;伦理投票编号Charité EA2/095/14。