Koster Geert, Bekema Hanneke J, Wetterslev Jørn, Gluud Christian, Keus Frederik, van der Horst Iwan C C
Department of Critical Care, University of Groningen, University Medical Centre Groningen, P.O. Box 30.001, 9700 RB, Groningen, The Netherlands.
Department of Anaesthesiology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands.
Intensive Care Med. 2016 Sep;42(9):1322-35. doi: 10.1007/s00134-016-4449-6. Epub 2016 Jul 22.
Milrinone is an inotrope widely used for treatment of cardiac failure. Because previous meta-analyses had methodological flaws, we decided to conduct a systematic review of the effect of milrinone in critically ill adult patients with cardiac dysfunction.
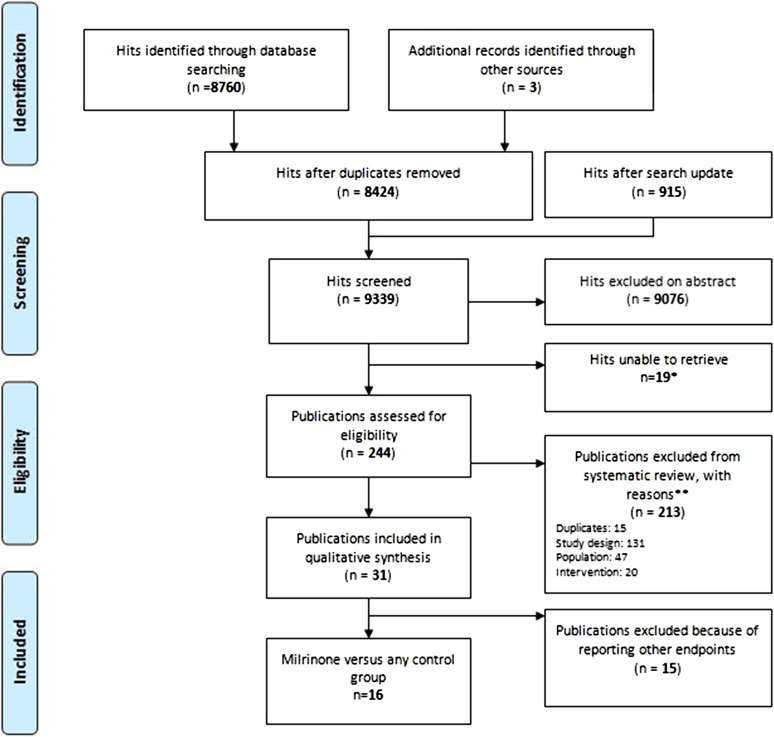
This systematic review was performed according to The Cochrane Handbook for Systematic Reviews of Interventions. Searches were conducted until November 2015. Patients with cardiac dysfunction were included. The primary outcome was serious adverse events (SAE) including mortality at maximum follow-up. The risk of bias was evaluated and trial sequential analyses were conducted. The quality of evidence was assessed by the Grading of Recommendations Assessment, Development and Evaluation criteria.
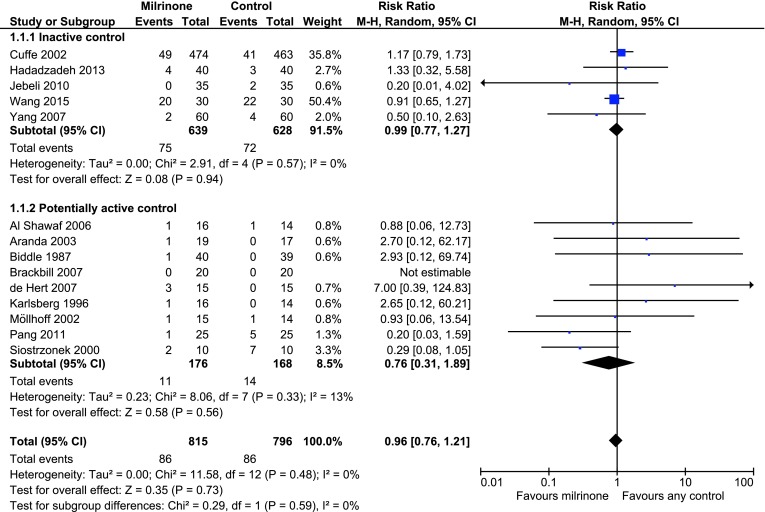
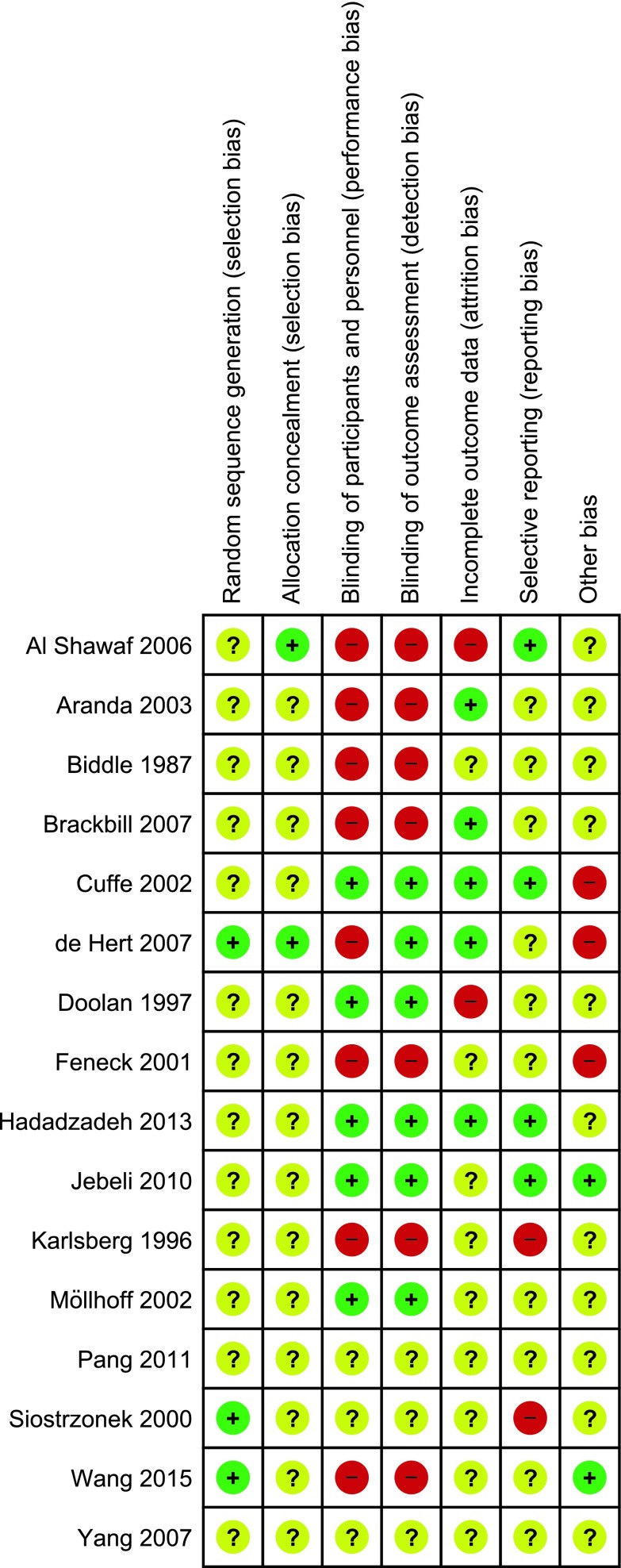
A total of 31 randomised clinical trials fulfilled the inclusion criteria, of which 16 provided data for our analyses. All trials were at high risk of bias, and none reported the primary composite outcome SAE. Fourteen trials with 1611 randomised patients reported mortality data at maximum follow-up (RR 0.96; 95% confidence interval 0.76-1.21). Milrinone did not significantly affect other patient-centred outcomes. All analyses displayed statistical and/or clinical heterogeneity of patients, interventions, comparators, outcomes, and/or settings and all featured missing data.
The current evidence on the use of milrinone in critically ill adult patients with cardiac dysfunction suffers from considerable risks of both bias and random error and demonstrates no benefits. The use of milrinone for the treatment of critically ill patients with cardiac dysfunction can be neither recommended nor refuted. Future randomised clinical trials need to be sufficiently large and designed to have low risk of bias.
米力农是一种广泛用于治疗心力衰竭的强心剂。由于先前的荟萃分析存在方法学缺陷,我们决定对米力农在成年重症心功能不全患者中的疗效进行系统评价。
本系统评价按照《Cochrane干预措施系统评价手册》进行。检索截至2015年11月。纳入心功能不全患者。主要结局为严重不良事件(SAE),包括最大随访期的死亡率。评估偏倚风险并进行试验序贯分析。采用推荐分级评估、制定和评价标准评估证据质量。
共有31项随机临床试验符合纳入标准,其中16项为我们的分析提供了数据。所有试验均存在高偏倚风险,且均未报告主要复合结局SAE。14项试验纳入1611例随机分组患者,报告了最大随访期的死亡率数据(风险比0.96;95%置信区间0.76 - 1.21)。米力农对其他以患者为中心的结局无显著影响。所有分析均显示患者、干预措施、对照、结局和/或研究背景存在统计学和/或临床异质性,且均存在数据缺失。
目前关于米力农在成年重症心功能不全患者中应用的证据存在相当大的偏倚风险和随机误差风险,且未显示出益处。既不推荐也不反对使用米力农治疗重症心功能不全患者。未来的随机临床试验需要足够大且设计为低偏倚风险。