Odsæter Ingrid Hov, Åsberg Arne, Vanky Eszter, Mørkved Siv, Stafne Signe Nilssen, Salvesen Kjell Åsmund, Carlsen Sven Magnus
Department of Clinical Chemistry, Clinic of Laboratory Medicine, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway ; Department of Cancer Research and Molecular Medicine, Faculty of Medicine, Norwegian University of Science and Technology, Trondheim, Norway.
Department of Clinical Chemistry, Clinic of Laboratory Medicine, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway.
Diabetol Metab Syndr. 2016 Jul 22;8:43. doi: 10.1186/s13098-016-0168-y. eCollection 2016.
Gestational diabetes mellitus (GDM) increases the risk for preeclampsia and macrosomia. GDM is conventionally diagnosed by an oral glucose tolerance test (OGTT). Hemoglobin A1c (HbA1c) is a marker for the average glucose level the last 2-3 months. We aimed to study if HbA1c alone or in combination with patient characteristics can be used to screen for GDM and reduce the number of OGTTs, and whether it could predict preeclampsia or birth weight.
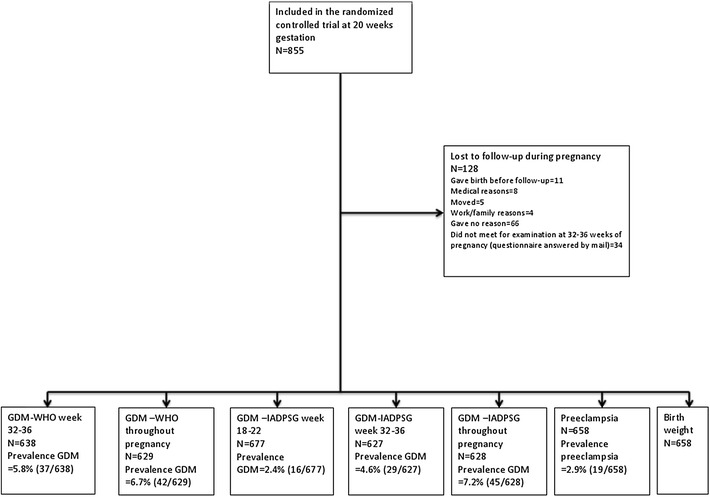
855 women from a previous study on the effect of exercise on GDM prevalence were eligible, whereof 677 were included. GDM was diagnosed by WHO 1999 criteria (GDM-WHO) and modified IADPSG criteria (GDM-IADPSG), at pregnancy weeks 18-22 and 32-36. HbA1c analyzed at pregnancy weeks 18-22 and 32-36, variables from patient history and clinical examination were considered for logistic regression models. The diagnostic accuracy was assessed by ROC curve analysis.
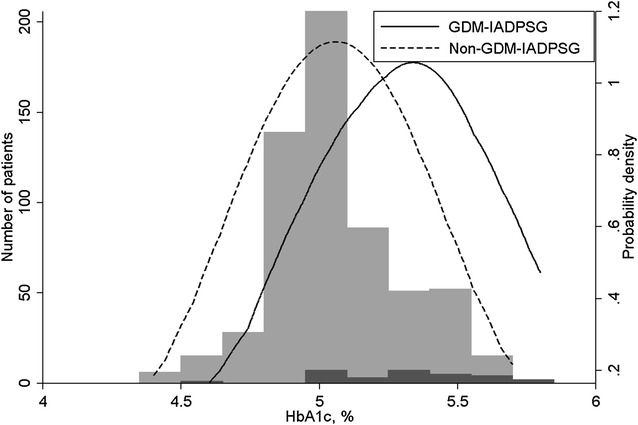
Accumulated GDM prevalence was 6.7 % by WHO and 7.2 % by modified IADPSG criteria. Nearly a third could potentially have avoided an OGTT by using HbA1c to exclude GDM-IADPSG with a sensitivity of 88 % at week 18-22 and 97 % at week 32-36. Further, 16 % could have avoided an OGTT with a sensitivity of 96 % using HbA1c at week 18-22 to exclude GDM-IADPSG throughout pregnancy. HbA1c was not accurate at diagnosing GDM-IADPSG, and it was inaccurate at screening for GDM-WHO at any time point. Adding other predictors did not increase the number of potentially avoidable OGTTs significantly. HbA1c was not significantly associated with preeclampsia or birth weight.
HbA1c could potentially reduce the number of OGTTs.
妊娠期糖尿病(GDM)会增加先兆子痫和巨大儿的风险。传统上,GDM通过口服葡萄糖耐量试验(OGTT)进行诊断。糖化血红蛋白(HbA1c)是过去2至3个月平均血糖水平的一个指标。我们旨在研究单独使用HbA1c或结合患者特征是否可用于筛查GDM并减少OGTT的次数,以及它是否能预测先兆子痫或出生体重。
来自先前一项关于运动对GDM患病率影响研究的855名女性符合条件,其中677名被纳入研究。在妊娠第18 - 22周和32 - 36周,根据世界卫生组织1999年标准(GDM - WHO)和改良的国际糖尿病与妊娠研究组(IADPSG)标准(GDM - IADPSG)诊断GDM。在妊娠第18 - 22周和32 - 36周分析HbA1c,将患者病史和临床检查的变量纳入逻辑回归模型。通过ROC曲线分析评估诊断准确性。
根据WHO标准,累积GDM患病率为6.7%,根据改良的IADPSG标准为7.2%。近三分之一的人通过使用HbA1c排除GDM - IADPSG有可能避免进行OGTT,在第18 - 22周时敏感性为88%,在第32 - 36周时为97%。此外,16%的人通过在第18 - 22周使用HbA1c排除整个孕期的GDM - IADPSG,敏感性为96%,有可能避免进行OGTT。HbA1c在诊断GDM - IADPSG时不准确,在任何时间点筛查GDM - WHO时也不准确。添加其他预测因素并未显著增加可能避免的OGTT次数。HbA1c与先兆子痫或出生体重无显著关联。
HbA1c有可能减少OGTT的次数。