Mizumori Yasuyuki, Nakahara Yasuharu, Kawamura Tetsuji, Sasaki Shin, Tsukamoto Hiroaki, Mochiduki Yoshiro
Department of Respiratory Medicine, National Hospital Organization, Himeji Medical Center, Hyogo, Japan.
J Bronchology Interv Pulmonol. 2016 Jul;23(3):199-203. doi: 10.1097/LBR.0000000000000289.
Bronchial occlusion therapy using silicon spigots is effective for intractable pneumothorax. However, sometimes the pneumothorax is refractory to bronchial occlusion because of collateral ventilation. For such difficult pneumothoraces, we attempted an intrabronchial infusion of autologous blood plus thrombin to control collateral ventilation and stop air leaks.
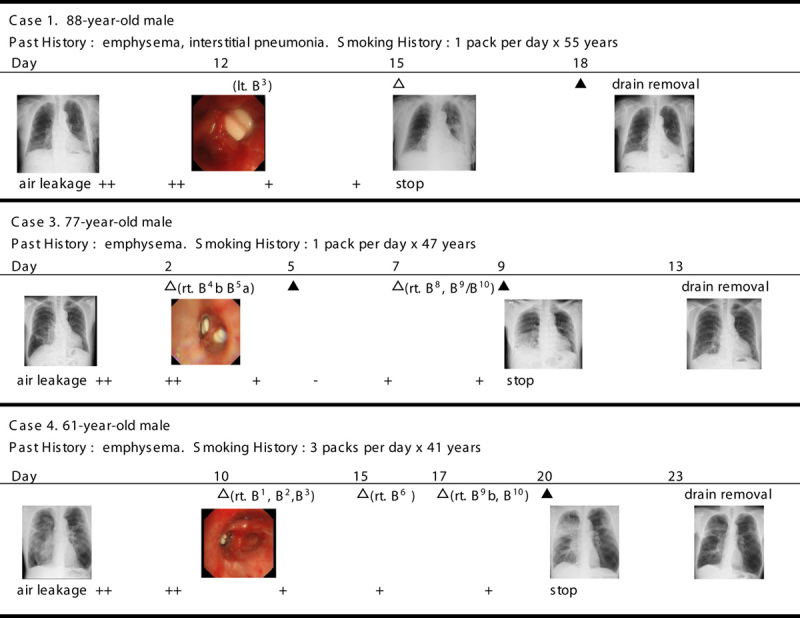
We performed bronchial occlusions using silicon spigots in patients with spontaneous pneumothorax secondary to emphysema and refractory to chest drainage, but which was inoperable owing to each patient's poor surgical candidacy and poor overall health condition. When bronchial occlusion proved ineffective, we undertook intrabronchial infusion of autologous blood plus thrombin, 2 to 4 days after bronchial occlusion. A catheter was inserted into the subpleural area, through a gap between the silicon spigot and the bronchial wall, using a flexible bronchoscope under fluoroscopic guidance. Autologous blood, followed by a thrombin solution, was infused using the catheter. We repeated the same infusion a total of 4 to 6 times while changing the target bronchi. All interventions were performed under local anesthesia.
The subjects were 9 men, aged from 61 to 88 years, with smoking histories. Three patients also had interstitial pneumonia, and 6 patients had undergone pleurodesis in vain before bronchial occlusion. For 4of the 9 patients, autologous blood plus thrombin infusions successfully stopped air leaks, and in 3 patients, intrabronchial infusions and pleurodesis halted leaks altogether.
Intrabronchial infusion of autologous blood plus thrombin was effective for intractable pneumothoraces that could not be clinically managed, even by bronchial occlusion using silicon spigots.
使用硅制插管进行支气管封堵治疗难治性气胸有效。然而,有时由于侧支通气,气胸对支气管封堵治疗无效。对于此类难治性气胸,我们尝试支气管内注入自体血加凝血酶以控制侧支通气并停止漏气。
我们对因肺气肿继发的自发性气胸且胸腔闭式引流无效,但因手术耐受性差和整体健康状况不佳而无法手术的患者,使用硅制插管进行支气管封堵。当支气管封堵证明无效时,在支气管封堵后2至4天,我们进行支气管内注入自体血加凝血酶。在透视引导下,使用可弯曲支气管镜通过硅制插管与支气管壁之间的间隙将导管插入胸膜下区域。使用导管注入自体血,随后注入凝血酶溶液。在更换目标支气管的同时,我们总共重复相同的注入4至6次。所有干预均在局部麻醉下进行。
研究对象为9名男性,年龄61至88岁,均有吸烟史。3例患者还患有间质性肺炎,6例患者在支气管封堵前胸膜固定术均失败。9例患者中有4例通过注入自体血加凝血酶成功停止漏气,3例患者通过支气管内注入和胸膜固定术完全停止漏气。
支气管内注入自体血加凝血酶对于即使使用硅制插管进行支气管封堵仍无法临床处理的难治性气胸有效。