Muth Christiane, Harder Sebastian, Uhlmann Lorenz, Rochon Justine, Fullerton Birgit, Güthlin Corina, Erler Antje, Beyer Martin, van den Akker Marjan, Perera Rafael, Knottnerus André, Valderas Jose M, Gerlach Ferdinand M, Haefeli Walter E
Institute of General Practice, Johann Wolfgang Goethe University, Frankfurt/Main, Germany.
Institute for Clinical Pharmacology, Johann Wolfgang Goethe University Hospital, Frankfurt/Main, Germany.
BMJ Open. 2016 Jul 25;6(7):e011613. doi: 10.1136/bmjopen-2016-011613.
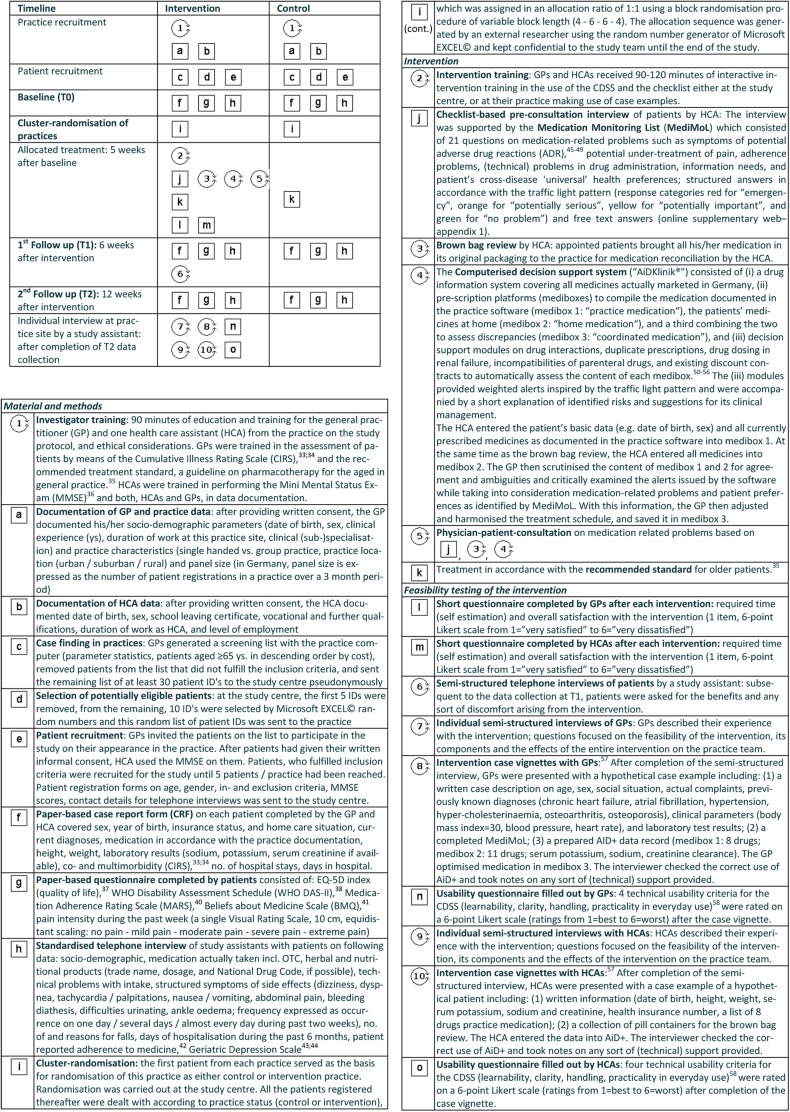
To improve medication appropriateness and adherence in elderly patients with multimorbidity, we developed a complex intervention involving general practitioners (GPs) and their healthcare assistants (HCA). In accordance with the Medical Research Council guidance on developing and evaluating complex interventions, we prepared for the main study by testing the feasibility of the intervention and study design in a cluster randomised pilot study.
20 general practices in Hesse, Germany.
100 cognitively intact patients ≥65 years with ≥3 chronic conditions, ≥5 chronic prescriptions and capable of participating in telephone interviews; 94 patients completed the study.
The HCA conducted a checklist-based interview with patients on medication-related problems and reconciled their medications. Assisted by a computerised decision-support system (CDSS), the GPs discussed medication intake with patients and adjusted their medication regimens. The control group continued with usual care.
Feasibility of the intervention and required time were assessed for GPs, HCAs and patients using mixed methods (questionnaires, interviews and case vignettes after completion of the study). The feasibility of the study was assessed concerning success of achieving recruitment targets, balancing cluster sizes and minimising drop-out rates. Exploratory outcomes included the medication appropriateness index (MAI), quality of life, functional status and adherence-related measures. MAI was evaluated blinded to group assignment, and intra-rater/inter-rater reliability was assessed for a subsample of prescriptions.
10 practices were randomised and analysed per group. GPs/HCAs were satisfied with the interventions despite the time required (35/45 min/patient). In case vignettes, GPs/HCAs needed help using the CDSS. The study made no patients feel uneasy. Intra-rater/inter-rater reliability for MAI was excellent. Inclusion criteria were challenging and potentially inadequate, and should therefore be adjusted. Outcome measures on pain, functionality and self-reported adherence were unfeasible due to frequent missing values, an incorrect manual or potentially invalid results.
Intervention and trial design were feasible. The pilot study revealed important limitations that influenced the design and conduct of the main study, thus highlighting the value of piloting complex interventions.
ISRCTN99691973; Results.
为提高患有多种疾病的老年患者用药的合理性及依从性,我们开展了一项涉及全科医生(GPs)及其医疗保健助理(HCAs)的综合干预措施。根据医学研究理事会关于开发和评估综合干预措施的指南,我们通过在一项整群随机试点研究中测试干预措施和研究设计的可行性,为主要研究做准备。
德国黑森州的20家全科诊所。
100名年龄≥65岁、患有≥3种慢性病、有≥5种慢性处方且能够参与电话访谈的认知功能完好的患者;94名患者完成了研究。
医疗保健助理就用药相关问题对患者进行基于检查表的访谈,并核对他们的用药情况。在计算机化决策支持系统(CDSS)的辅助下,全科医生与患者讨论用药情况并调整其用药方案。对照组继续接受常规护理。
采用混合方法(研究结束后通过问卷调查、访谈和病例 vignettes)对全科医生、医疗保健助理和患者评估干预措施的可行性及所需时间。从实现招募目标、平衡整群规模和尽量降低失访率方面评估研究的可行性。探索性指标包括用药合理性指数(MAI)、生活质量、功能状态和与依从性相关的指标。MAI在对分组不知情的情况下进行评估,并对一部分处方样本评估评分者内/评分者间的可靠性。
每组随机选取10家诊所进行分析。尽管需要一定时间(每位患者35/45分钟),全科医生/医疗保健助理对干预措施感到满意。在病例 vignettes 中,全科医生/医疗保健助理在使用CDSS时需要帮助。该研究没有让任何患者感到不安。MAI的评分者内/评分者间可靠性极佳。纳入标准具有挑战性且可能不充分,因此应进行调整。由于频繁出现缺失值、手册不正确或结果可能无效,关于疼痛、功能和自我报告的依从性的观察指标不可行。
干预措施和试验设计是可行的。试点研究揭示了影响主要研究设计和实施的重要局限性,从而凸显了对综合干预措施进行试点的价值。
ISRCTN99691973;结果