Orde Sam R, Boon Andrea J, Firth Daniel G, Villarraga Hector R, Sekiguchi Hiroshi
Division of Cardiovascular Diseases, Mayo Clinic, Rochester, Minnesota, USA.
Department of Intensive Care, Nepean Hospital, Sydney, Australia.
BMC Anesthesiol. 2016 Jul 25;16(1):43. doi: 10.1186/s12871-016-0201-6.
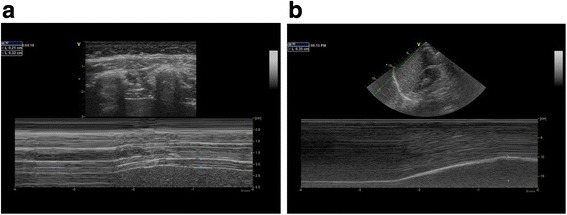
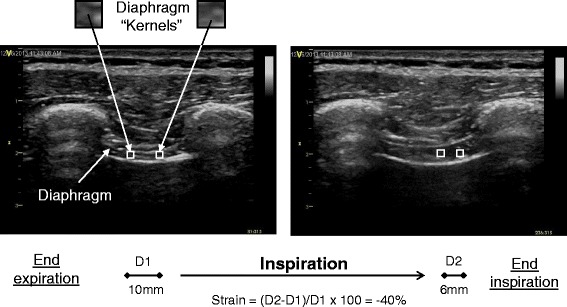
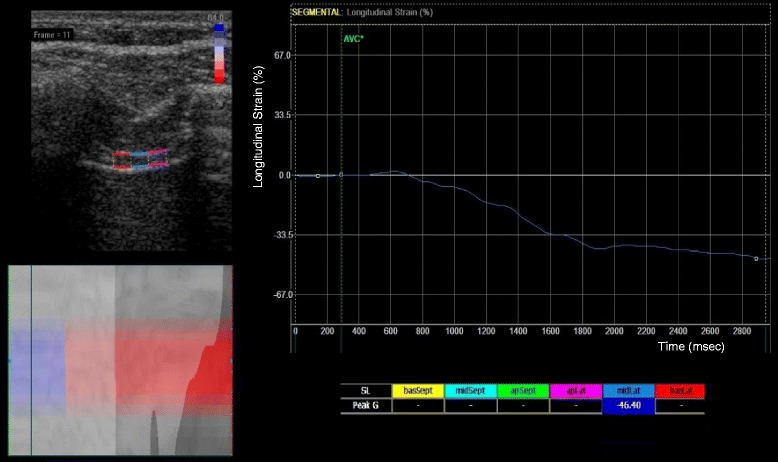
Conventionally, ultrasonographic assessment of diaphragm contractility has involved measuring respiratory changes in diaphragm thickness (thickening fraction) using B-mode or caudal displacement with M-mode. Two-dimensional speckle-tracking has been increasingly used to assess muscle deformation ('strain') in echocardiography. We sought to determine in a pilot study if this technology could be utilized to analyze diaphragmatic contraction.
Fifty healthy adult volunteers with normal exercise capacity underwent ultrasound imaging. A linear array transducer was used for the assessment of diaphragm thickness, thickening fraction (TF), and strain in the right anterior axillary line at approximately the ninth intercostal space. A phased array transducer was applied subcostally for the assessment of diaphragm displacement on the right mid-clavicular line. Diaphragmatic images were recorded from the end of expiration through the end of inspiration at 60 % maximal inspiratory capacity. Diaphragm strain was analyzed off-line by speckle tracking imaging. Blinded inter- and intra-rater variability was tested in 10 cases.
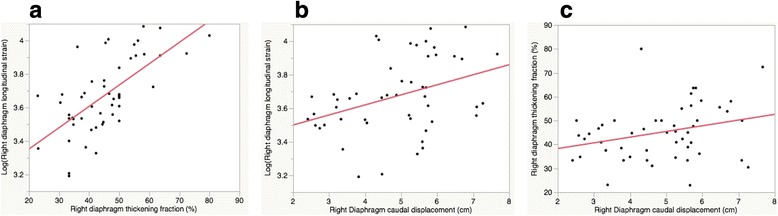
Mean right diaphragm thickness at end-expiration (±SD: standard deviation) was 0.24 cm (±0.1), with TF of 45.1 % (±12) at 60 % peak inspiratory effort. Mean right diaphragm caudal displacement was 4.9 cm (±1). Mean right diaphragm strain was -40.3 % (±9). A moderate correlation was seen between longitudinal strain and TF (R(2) 0.44, p < 0.0001). A weak correlation was seen between strain and caudal displacement (R(2) 0.14, p < 0.01), and an even weaker correlation was seen between caudal displacement and TF (R(2) 0.1, p = 0.04). Age, gender, and body mass index were not significantly associated with right diaphragm strain or TF. Although inter- and intra-rater variability was overall good for TF, caudal displacement, and strain (inter-rater R(2); 0.8, 0.9, and 0.7, respectively [p < 0.01], intra-rater R(2); 0.9, 0.7, and 0.9, respectively [p < 0.01]), strain values did have a slightly lower inter-rater repeatability.
Diaphragmatic strain estimated by speckle tracking imaging was associated with conventional ultrasound measures of diaphragmatic function (TF and caudal displacement). Further clinical studies are warranted to investigate its clinical utility.
传统上,超声评估膈肌收缩功能涉及使用B模式测量膈肌厚度的呼吸变化(增厚率)或使用M模式测量膈肌尾端位移。二维斑点追踪技术在超声心动图中越来越多地用于评估心肌变形(“应变”)。我们试图在一项初步研究中确定该技术是否可用于分析膈肌收缩。
50名运动能力正常的健康成年志愿者接受了超声成像检查。使用线性阵列换能器在右腋前线大约第9肋间评估膈肌厚度、增厚率(TF)和应变。使用相控阵换能器在右锁骨中线肋下评估膈肌位移。在60%最大吸气量时,从呼气末到吸气末记录膈肌图像。通过斑点追踪成像离线分析膈肌应变。对10例病例进行了评分者间和评分者内的盲法变异性测试。
呼气末右膈肌平均厚度(±标准差)为0.24cm(±0.1),在60%吸气峰值时TF为45.1%(±12)。右膈肌平均尾端位移为4.9cm(±1)。右膈肌平均应变是-40.3%(±9)。纵向应变与TF之间存在中度相关性(R² 0.44,p<0.0001)。应变与尾端位移之间存在弱相关性(R² 0.14,p<0.01),尾端位移与TF之间的相关性更弱(R² 0.1,p = 0.04)。年龄、性别和体重指数与右膈肌应变或TF无显著相关性。虽然评分者间和评分者内变异性对于TF、尾端位移和应变总体良好(评分者间R²分别为0.8、0.9和0.7 [p<0.01],评分者内R²分别为0.9、0.7和0.9 [p<0.01]),但应变值的评分者间重复性略低。
通过斑点追踪成像估计的膈肌应变与膈肌功能的传统超声测量指标(TF和尾端位移)相关。有必要进行进一步的临床研究以探讨其临床应用价值。