Cunnane Stephen C, Courchesne-Loyer Alexandre, Vandenberghe Camille, St-Pierre Valérie, Fortier Mélanie, Hennebelle Marie, Croteau Etienne, Bocti Christian, Fulop Tamas, Castellano Christian-Alexandre
Research Center on Aging, SherbrookeQC, Canada; Department of Medicine, Université de Sherbrooke, SherbrookeQC, Canada; Department of Pharmacology and Physiology, Université de Sherbrooke, SherbrookeQC, Canada.
Research Center on Aging, SherbrookeQC, Canada; Department of Pharmacology and Physiology, Université de Sherbrooke, SherbrookeQC, Canada.
Front Mol Neurosci. 2016 Jul 8;9:53. doi: 10.3389/fnmol.2016.00053. eCollection 2016.
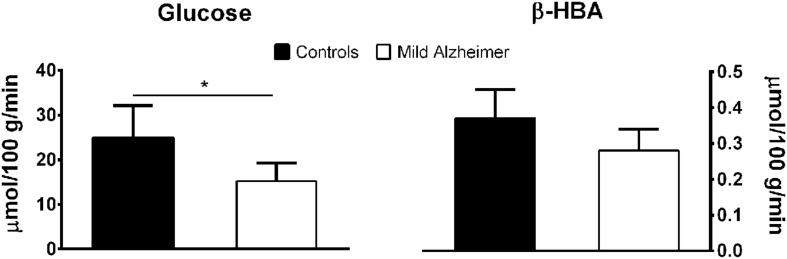
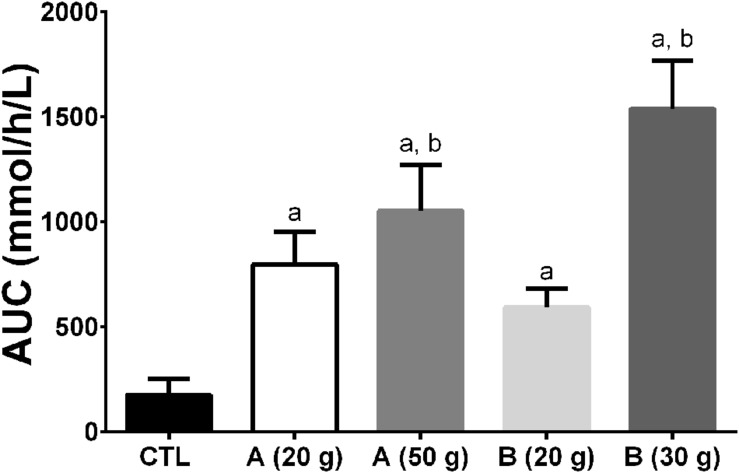
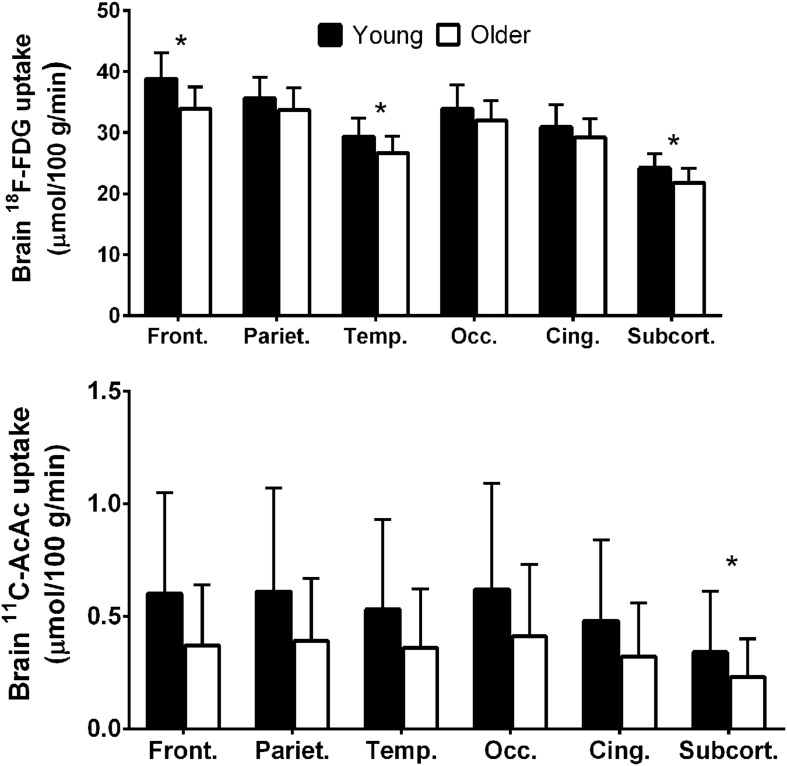
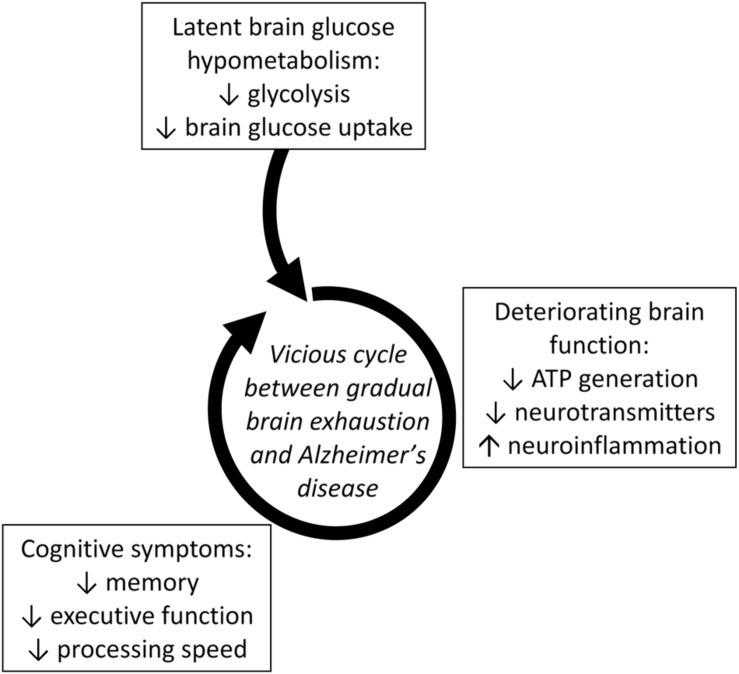
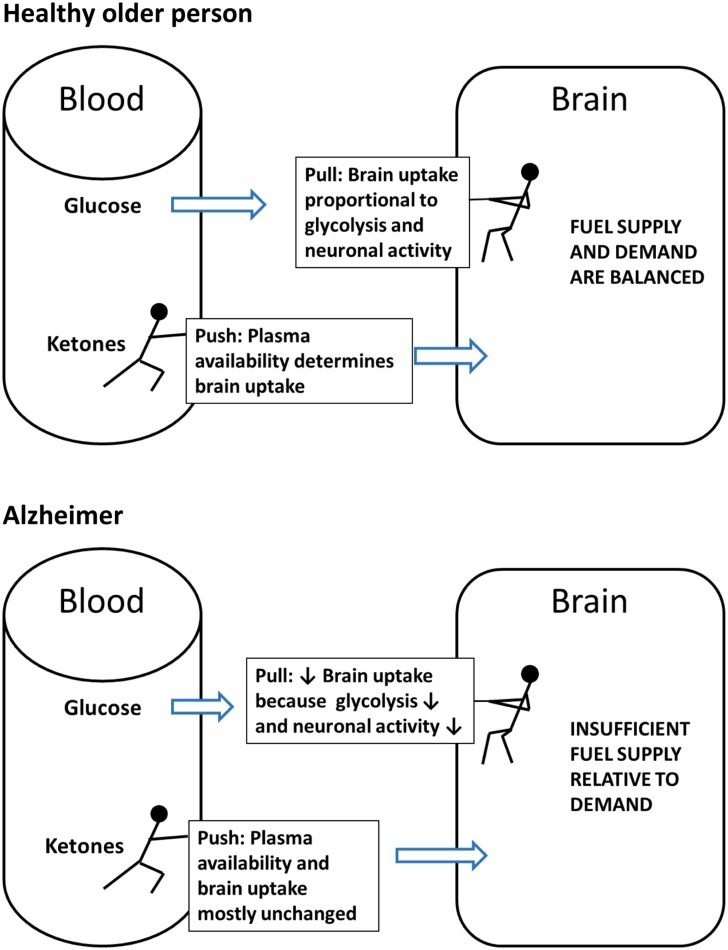
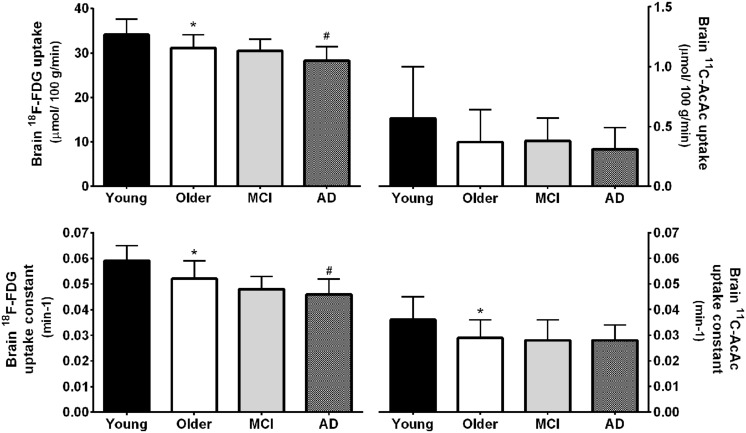
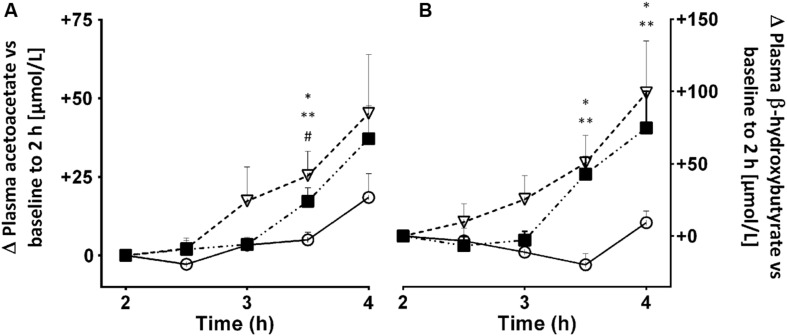
We propose that brain energy deficit is an important pre-symptomatic feature of Alzheimer's disease (AD) that requires closer attention in the development of AD therapeutics. Our rationale is fourfold: (i) Glucose uptake is lower in the frontal cortex of people >65 years-old despite cognitive scores that are normal for age. (ii) The regional deficit in brain glucose uptake is present in adults <40 years-old who have genetic or lifestyle risk factors for AD but in whom cognitive decline has not yet started. Examples include young adult carriers of presenilin-1 or apolipoprotein E4, and young adults with mild insulin resistance or with a maternal family history of AD. (iii) Regional brain glucose uptake is impaired in AD and mild cognitive impairment (MCI), but brain uptake of ketones (beta-hydroxybutyrate and acetoacetate), remains the same in AD and MCI as in cognitively healthy age-matched controls. These observations point to a brain fuel deficit which appears to be specific to glucose, precedes cognitive decline associated with AD, and becomes more severe as MCI progresses toward AD. Since glucose is the brain's main fuel, we suggest that gradual brain glucose exhaustion is contributing significantly to the onset or progression of AD. (iv) Interventions that raise ketone availability to the brain improve cognitive outcomes in both MCI and AD as well as in acute experimental hypoglycemia. Ketones are the brain's main alternative fuel to glucose and brain ketone uptake is still normal in MCI and in early AD, which would help explain why ketogenic interventions improve some cognitive outcomes in MCI and AD. We suggest that the brain energy deficit needs to be overcome in order to successfully develop more effective therapeutics for AD. At present, oral ketogenic supplements are the most promising means of achieving this goal.
我们提出,脑能量不足是阿尔茨海默病(AD)的一个重要症状前特征,在AD治疗学的发展中需要更密切关注。我们的理由有四点:(i)65岁以上人群额叶皮质的葡萄糖摄取较低,尽管其认知评分在年龄上是正常的。(ii)在40岁以下有AD遗传或生活方式风险因素但认知功能尚未开始下降的成年人中存在脑葡萄糖摄取的区域缺陷。例子包括早老素-1或载脂蛋白E4的年轻成年携带者,以及有轻度胰岛素抵抗或有AD母系家族史的年轻人。(iii)AD和轻度认知障碍(MCI)患者的脑区域葡萄糖摄取受损,但AD和MCI患者的脑酮(β-羟基丁酸和乙酰乙酸)摄取与认知健康的年龄匹配对照组相同。这些观察结果表明存在脑燃料不足,这似乎是葡萄糖特有的,先于与AD相关的认知下降,并随着MCI向AD进展而变得更严重。由于葡萄糖是大脑的主要燃料,我们认为脑葡萄糖逐渐耗尽对AD的发生或进展有显著影响。(iv)提高脑酮可用性的干预措施可改善MCI和AD患者以及急性实验性低血糖患者的认知结果。酮是大脑葡萄糖的主要替代燃料,MCI和早期AD患者的脑酮摄取仍然正常,这有助于解释为什么生酮干预可改善MCI和AD患者的一些认知结果。我们认为,为了成功开发更有效的AD治疗方法,需要克服脑能量不足。目前,口服生酮补充剂是实现这一目标最有前景的手段。