Bozzani Fiammetta Maria, Arnold Matthias, Colbourn Timothy, Lufesi Norman, Nambiar Bejoy, Masache Gibson, Skordis-Worrall Jolene
Department of Global Health and Development, London School of Hygiene & Tropical Medicine, 15-17 Tavistock Place, London, WC1H 9SH, UK.
Institute for Global Health, University College London, London, UK.
BMC Health Serv Res. 2016 Jul 28;16:314. doi: 10.1186/s12913-016-1573-5.
Human resources are a major cost driver in childhood pneumonia case management. Introduction of 13-valent pneumococcal conjugate vaccine (PCV-13) in Malawi can lead to savings on staff time and salaries due to reductions in pneumonia cases requiring admission. Reliable estimates of human resource costs are vital for use in economic evaluations of PCV-13 introduction.
Twenty-eight severe and twenty-four very severe pneumonia inpatients under the age of five were tracked from admission to discharge by paediatric ward staff using self-administered timesheets at Mchinji District Hospital between June and August 2012. All activities performed and the time spent on each activity were recorded. A monetary value was assigned to the time by allocating a corresponding percentage of the health workers' salary. All costs are reported in 2012 US$.
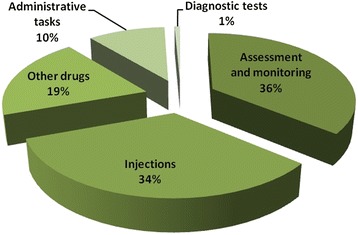
A total of 1,017 entries, grouped according to 22 different activity labels, were recorded during the observation period. On average, 99 min (standard deviation, SD = 46) were spent on each admission: 93 (SD = 38) for severe and 106 (SD = 55) for very severe cases. Approximately 40 % of activities involved monitoring and stabilization, including administering non-drug therapies such as oxygen. A further 35 % of the time was spent on injecting antibiotics. Nurses provided 60 % of the total time spent on pneumonia admissions, clinicians 25 % and support staff 15 %. Human resource costs were approximately US$ 2 per bed-day and, on average, US$ 29.5 per severe pneumonia admission and US$ 37.7 per very severe admission.
Self-reporting was successfully used in this context to generate reliable estimates of human resource time and costs of childhood pneumonia treatment. Assuming vaccine efficacy of 41 % and 90 % coverage, PCV-13 introduction in Malawi can save over US$ 2 million per year in staff costs alone.
人力资源是儿童肺炎病例管理中的主要成本驱动因素。在马拉维引入13价肺炎球菌结合疫苗(PCV - 13)可因需要住院治疗的肺炎病例减少而节省工作人员时间和工资。可靠的人力资源成本估计对于PCV - 13引入的经济评估至关重要。
2012年6月至8月期间,姆钦吉区医院的儿科病房工作人员使用自行填写的时间表,对28名5岁以下的重症肺炎住院患者和24名极重症肺炎住院患者从入院到出院进行了跟踪。记录了所有执行的活动以及每项活动所花费的时间。通过分配卫生工作者工资的相应百分比来为时间赋予货币价值。所有成本均以2012年美元报告。
在观察期内共记录了1017条记录,根据22个不同的活动标签进行分组。每次入院平均花费99分钟(标准差,SD = 46):重症病例为93分钟(SD = 38),极重症病例为106分钟(SD = 55)。大约40%的活动涉及监测和稳定病情,包括给予非药物治疗,如输氧。另外35%的时间用于注射抗生素。护士提供了肺炎入院总时间的60%,临床医生提供了25%,辅助人员提供了15%。人力资源成本约为每天每张床位2美元,重症肺炎入院平均为29.5美元,极重症入院平均为37.7美元。
在这种情况下,自我报告成功用于生成儿童肺炎治疗的人力资源时间和成本的可靠估计。假设疫苗效力为41%且覆盖率为90%,在马拉维引入PCV - 13仅在工作人员成本方面每年就可节省超过200万美元。