Jarosz Anna, Darocha Tomasz, Kosiński Sylweriusz, Gałązkowski Robert, Mazur Piotr, Piątek Jacek, Konstanty-Kalandyk Janusz, Hymczak Hubert, Drwiła Rafał
From the *Department of Anesthesiology and Intensive Care, The John Paul II Hospital, Krakow, Poland; †Institute of Cardiology, Jagiellonian University Medical College, Krakow, Poland; ‡Department of Anesthesiology and Intensive Care, Pulmonary Hospital, Zakopane, Poland; §Tatra Mountain Rescue Service, Zakopane, Poland; ¶Department of Emergency Medical Services, Medical University of Warsaw, Warsaw, Poland; ‖Polish Medical Air Rescue, Warsaw, Poland; and #Department of Cardiovascular Surgery and Transplantology, The John Paul II Hospital, Krakow, Poland.
ASAIO J. 2017 May/Jun;63(3):e26-e30. doi: 10.1097/MAT.0000000000000422.
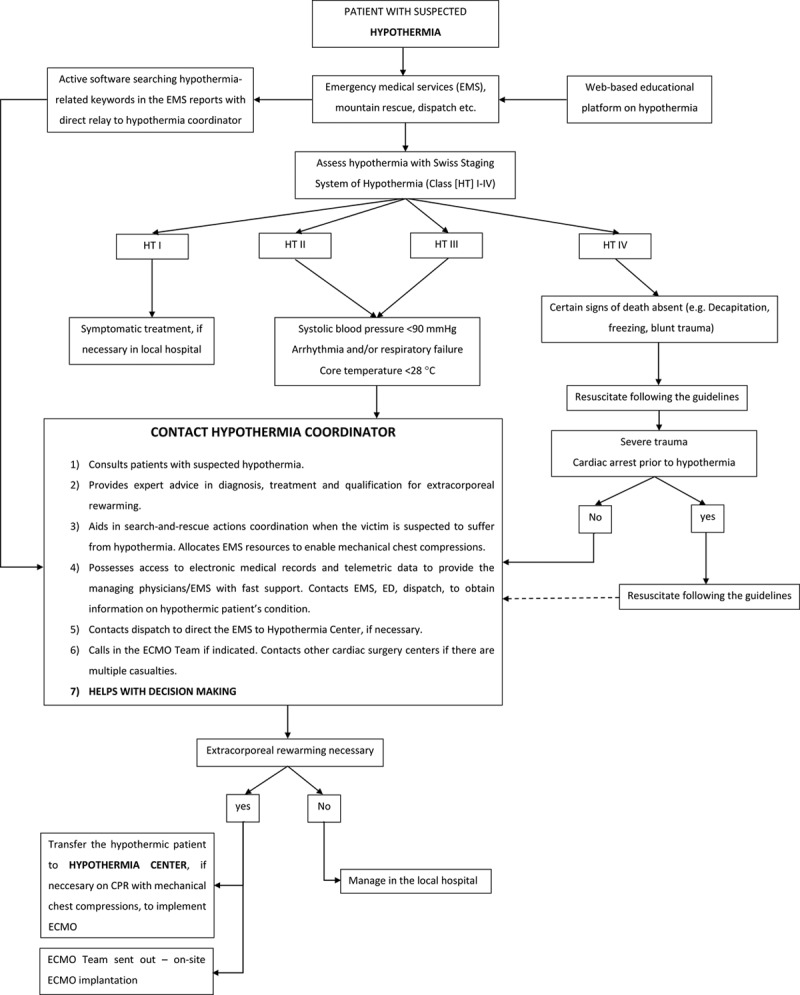
We sought to organize a functional system of recognition and advanced treatment of hypothermic patients with extracorporeal rewarming as a treatment option. All patients with suspected hypothermia are consulted with the hypothermia coordinator (HC), whose role is to provide expertise on hypothermia recognition and treatment to all rescue and medical services. Patients with Swiss staging system of hypothermia class III and IV are subjected to extracorporeal rewarming. Patients with class I and II are managed in local hospitals, after the HC provides instructions. From program initiation (July 29, 2013) to November 1, 2015, HC consulted 104 hypothermic patients; 21 in hypothermia class III and IV were subjected to extracorporeal rewarming in the John Paul II Hospital in Cracow, Poland. The remaining people were rewarmed in the referring hospitals. Cardiac arrest upon referral was present in 10 cases (resuscitation times from arrest to extracorporeal membrane oxygenation implantation ranged 107-345 minutes). Seven patients died, and the remaining 14 have been rewarmed with the restoration of hemodynamic stability. Systematic approach to active recognition and treatment of profound accidental hypothermia patients, on the basis of HC cooperation with emergency medical services, enables advanced management with good outcomes, especially in patients with cardiac arrest.
我们试图构建一个功能系统,用于识别体温过低患者并将体外复温作为一种治疗选择进行高级治疗。所有疑似体温过低的患者都会咨询体温过低协调员(HC),其职责是为所有救援和医疗服务提供体温过低识别与治疗方面的专业知识。瑞士低温分期系统III级和IV级的患者接受体外复温。I级和II级患者在HC提供指导后,在当地医院接受治疗。从项目启动(2013年7月29日)到2015年11月1日,HC咨询了104名体温过低患者;其中21名III级和IV级低温患者在波兰克拉科夫的约翰·保罗二世医院接受了体外复温。其余患者在转诊医院进行复温。转诊时出现心脏骤停的有10例(从心脏骤停到植入体外膜肺氧合的复苏时间为107 - 345分钟)。7名患者死亡,其余14名患者已复温且血流动力学稳定性恢复。基于HC与紧急医疗服务的合作,对严重意外低温患者进行积极识别和治疗的系统方法能够实现良好的高级管理效果,尤其是对于心脏骤停患者。