Nakstad Britt, Sonerud Tonje, Solevåg Anne Lee
Department of Pediatric and Adolescent Medicine, Akershus University Hospital, Lørenskog; Institute of Clinical Medicine, University of Oslo, Lørenskog.
Department of Pediatric and Adolescent Medicine, Akershus University Hospital, Lørenskog; Section of Clinical Molecular Biology (EpiGen), Division of Medicine, Akershus University Hospital, Lørenskog, Norway.
Infect Drug Resist. 2016 Jul 8;9:171-9. doi: 10.2147/IDR.S106181. eCollection 2016.
Group B streptococcus (GBS) infection remains a major cause of neonatal morbidity and mortality, and GBS III is the predominant strain in early-onset GBS neonatal sepsis. To avoid both over- and undertreatment of infants with nonspecific signs of infection, early diagnostic tools are warranted. The aim of this study was to identify biomarkers with high sensitivity and specificity in an early stage of GBS infection. A secondary aim was to assess the utility of a human umbilical cord blood (HUCB) model system of early-onset neonatal sepsis.
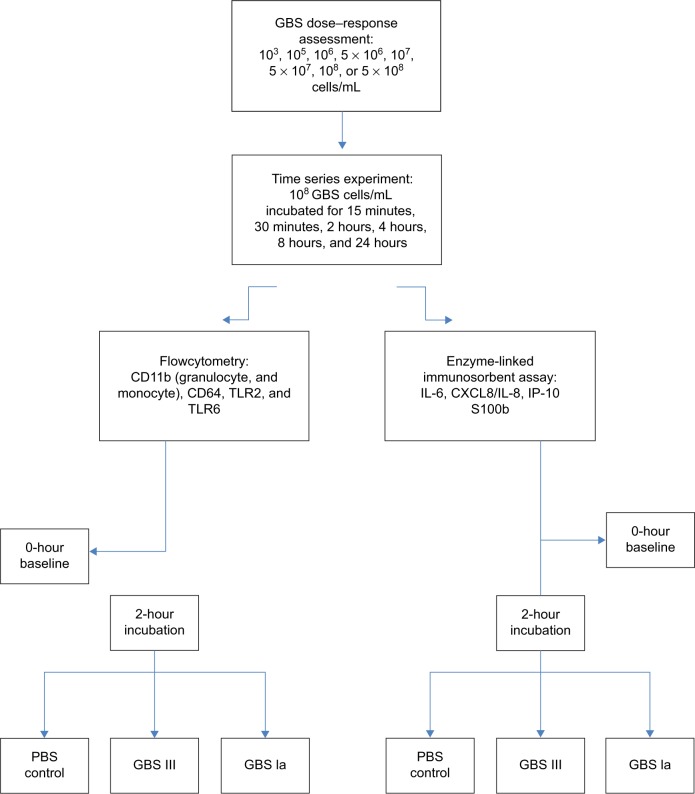
Umbilical cord blood samples from 20 healthy term pregnancies were stimulated for 2 hours with a GBS III isolate from a patient and a commercially available GBS Ia strain. Nonstimulated samples served as controls. Leukocyte surface markers (CD11b, CD64, toll-like receptor [TLR] 2, TLR4, and TLR6) were analyzed by flow cytometry and soluble biomarkers by enzyme-linked immunosorbent assay (interleukin [IL]-6 and -8; interferon-γ-inducing protein [IP]-10; and S100b). The area under the receiver operating characteristic curve (AUC) was calculated for the markers.
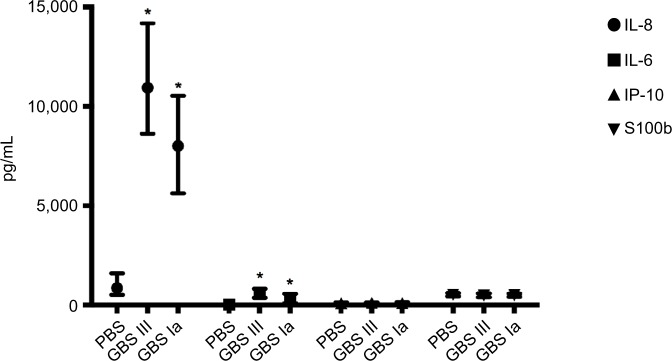
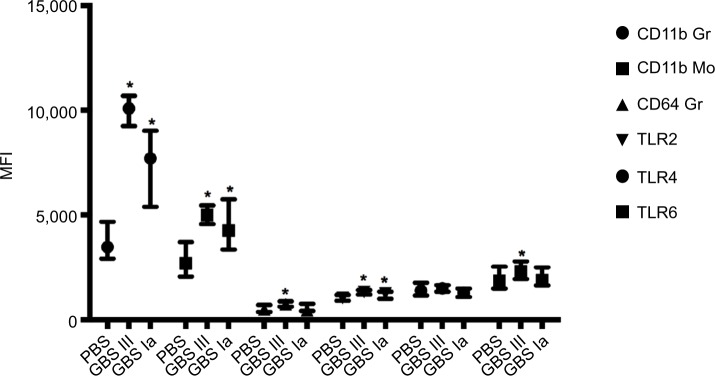
GBS III gave the highest responses and AUC values for all biomarkers. Only IL-6 and IL-8 displayed an AUC approaching 0.8 for both GBS serotypes (P<0.001). IL-8 >5,292 pg/mL had both a sensitivity and a specificity of 1.00. IL-6 >197 pg/mL had both a sensitivity and a specificity of 0.95 for GBS III stimulation. CD11b on granulocytes and monocytes was the leukocyte surface marker with the highest AUC values for both GBS serotypes.
In agreement with previous studies, IL-6, IL-8, and potentially CD11b could be useful in diagnosing neonatal GBS infection in an early stage. Our HUCB early-onset neonatal sepsis model may be useful for evaluating biomarkers of neonatal sepsis. The HUCB of neonates with risk factors for sepsis might even be used for diagnostic purposes, but requires further study.
B族链球菌(GBS)感染仍是新生儿发病和死亡的主要原因,GBS III是早发型GBS新生儿败血症的主要菌株。为避免对有非特异性感染体征的婴儿进行过度治疗和治疗不足,需要早期诊断工具。本研究的目的是在GBS感染早期识别具有高敏感性和特异性的生物标志物。次要目的是评估早发型新生儿败血症的人脐带血(HUCB)模型系统的效用。
用来自一名患者的GBS III分离株和一种市售的GBS Ia菌株对20例健康足月妊娠的脐带血样本进行2小时刺激。未刺激的样本用作对照。通过流式细胞术分析白细胞表面标志物(CD11b、CD64、Toll样受体[TLR]2、TLR4和TLR6),并通过酶联免疫吸附测定分析可溶性生物标志物(白细胞介素[IL]-6和-8;干扰素-γ诱导蛋白[IP]-10;以及S100b)。计算标志物的受试者工作特征曲线下面积(AUC)。
GBS III对所有生物标志物的反应和AUC值最高。仅IL-6和IL-8对两种GBS血清型的AUC均接近0.8(P<0.001)。IL-8>5292 pg/mL的敏感性和特异性均为1.00。对于GBS III刺激,IL-6>197 pg/mL的敏感性和特异性均为0.95。粒细胞和单核细胞上的CD11b是两种GBS血清型中AUC值最高的白细胞表面标志物。
与先前的研究一致,IL-6、IL-8以及可能的CD11b可用于早期诊断新生儿GBS感染。我们的HUCB早发型新生儿败血症模型可能有助于评估新生儿败血症的生物标志物。有败血症危险因素的新生儿的HUCB甚至可能用于诊断目的,但需要进一步研究。