Marconi Daniel Grossi, Fregnani Jose Humberto Tavares Guerreiro, Rossini Rodrigo Ribeiro, Netto Ana Karina Borges Junqueira, Lucchesi Fabiano Rubião, Tsunoda Audrey Tieko, Kamrava Mitchell
Department of Radiation Oncology, Barretos Cancer Hospital, Antenor Duarte Villela, 1331, Barretos, Sao Paulo, 14784-400, Brazil.
Department of Gynecology Oncology, Barretos Cancer Hospital, Barretos, Sao Paulo, Brazil.
BMC Cancer. 2016 Jul 28;16:556. doi: 10.1186/s12885-016-2619-0.
Diffusion Weighted (DW) Magnetic Resonance Imaging (MRI) has been studed in several cancers including cervical cancer. This study was designed to investigate the association of DW-MRI parameters with baseline clinical features and clinical outcomes (local regional control (LRC), disease free survival (DFS) and disease specific survival (DSS)) in cervical cancer patients treated with definitive chemoradiation.
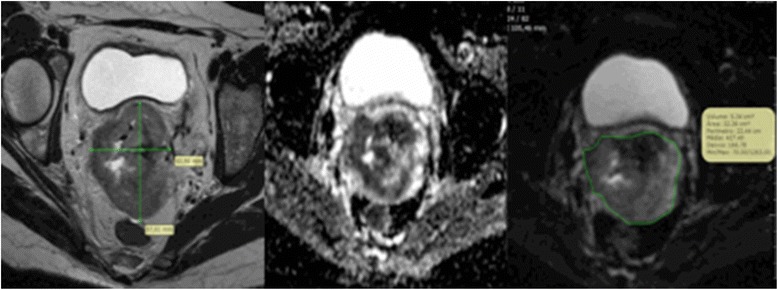
This was a retrospective study approved by an institutional review board that included 66 women with cervical cancer treated with definitive chemoradiation who underwent pre-treatment MRI at our institution between 2012 and 2013. A region of interest (ROI) was manually drawn by one of three radiologists with experience in pelvic imaging on a single axial CT slice encompassing the widest diameter of the cervical tumor while excluding areas of necrosis. The following apparent diffusion coefficient (ADC) values (×10(-3) mm(2)/s) were extracted for each ROI: Minimum - ADCmin, Maximum - ADCmax, Mean - ADCmean, and Standard Deviation of the ADC - ADCdev. Receiver operating characteristic (ROC) curves were built to choose the most accurate cut off value for each ADC value. Correlation between imaging metrics and baseline clinical features were evaluated using the Mann Whitney test. Confirmatory multi-variate Cox modeling was used to test associations with LRC (adjusted by gross tumor volume - GTV), DFS and DSS (both adjusted by FIGO stage). Kaplan Meyer curves were built for DFS and DSS. A p-value < 0.05 was considered significant. Women median age was 52 years (range 23-90). 67 % had FIGO stage I-II disease while 33 % had FIGO stage III-IV disease. Eighty-two percent had squamous cell cancer. Eighty-eight percent received concurrent cisplatin chemotherapy with radiation. Median EQD2 of external beam and brachytherapy was 82.2 Gy (range 74-84).
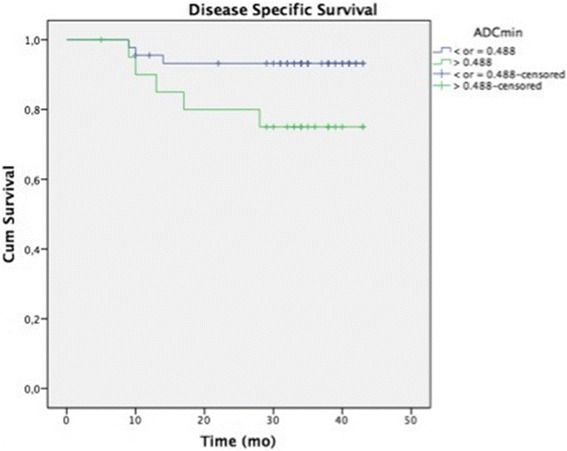
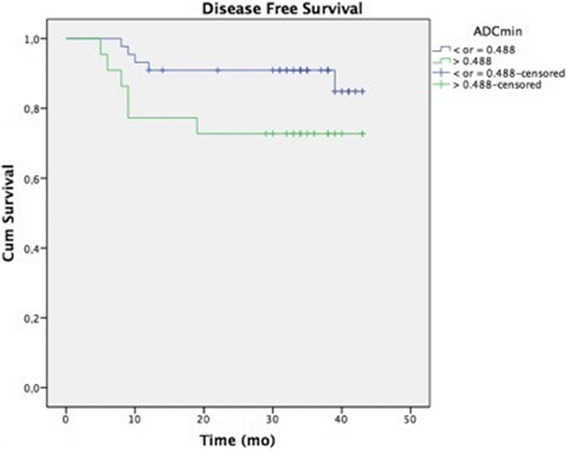
Women with disease staged III-IV (FIGO) had significantly higher mean ADCmax values compared with those with stage I-II (1.806 (0.4) vs 1.485 (0.4), p = 0.01). Patients with imaging defined positive nodes also had significantly higher mean (±SD) ADCmax values compared with lymph node negative patients (1.995 (0.3) vs 1.551 (0.5), p = 0.03). With a median follow-up of 32 months (range 5-43) 11 patients (17 %) have developed recurrent disease and 8 (12 %) have died because of cervical cancer. ROC curves based on DSS showed optimal cutoffs for ADCmin (0.488 × 10(-3)), ADCmean (0.827 × 10(-3)), ADCmax (1.838 × 10(-3)) and ADCdev (0.148 × 10(-3)). ADCmin higher than the cutoff was significantly associated with worse DFS (HR = 3.632-95 % CI: 1.094-12.054; p = 0.035) and DSS (HR = 4.401-95 % CI: 1.048-18.483; p = 0.043).
Pre-treatment ADCmax measured in the primary tumor may be associated with FIGO stage and lymph node status. Pre-treatment ADCmin may be a prognostic factor associated with disease-free survival and disease-specific survival in cervical cancer patients treated with definitive chemoradiation. Prospective validation of these findings is currently ongoing.
扩散加权磁共振成像(DW-MRI)已在包括宫颈癌在内的多种癌症中得到研究。本研究旨在探讨DW-MRI参数与接受根治性放化疗的宫颈癌患者的基线临床特征及临床结局(局部区域控制(LRC)、无病生存期(DFS)和疾病特异性生存期(DSS))之间的关联。
这是一项经机构审查委员会批准的回顾性研究,纳入了66例接受根治性放化疗的宫颈癌女性患者,她们于2012年至2013年在本机构接受了治疗前MRI检查。由三位具有盆腔成像经验的放射科医生之一在包含宫颈肿瘤最大直径的单个轴向CT切片上手动绘制感兴趣区域(ROI),同时排除坏死区域。为每个ROI提取以下表观扩散系数(ADC)值(×10⁻³mm²/s):最小值-ADCmin、最大值-ADCmax、平均值-ADCmean以及ADC的标准差-ADCdev。构建受试者操作特征(ROC)曲线以选择每个ADC值的最准确临界值。使用Mann-Whitney检验评估成像指标与基线临床特征之间的相关性。采用验证性多变量Cox模型来检验与LRC(根据大体肿瘤体积-GTV进行调整)、DFS和DSS(均根据国际妇产科联盟(FIGO)分期进行调整)的关联。为DFS和DSS构建Kaplan-Meier曲线。p值<0.05被认为具有统计学意义。女性患者的中位年龄为52岁(范围23 - 90岁)。67%为FIGO I-II期疾病,而33%为FIGO III-IV期疾病。82%为鳞状细胞癌。88%接受了顺铂同步放化疗。外照射和近距离放疗的中位等效剂量(EQD2)为82.2 Gy(范围74 - 84)。
FIGO III-IV期疾病的女性患者的平均ADCmax值显著高于I-II期患者(1.806(0.4)对1.485(0.4),p = 0.01)。影像学定义为阳性淋巴结的患者的平均(±标准差)ADCmax值也显著高于淋巴结阴性患者(1.995(0.3)对1.551(0.5),p = 0.03)。中位随访32个月(范围5 - 43个月),11例患者(17%)出现疾病复发,8例(12%)因宫颈癌死亡。基于DSS的ROC曲线显示ADCmin(0.488×10⁻³)、ADCmean(0.827×10⁻³)、ADCmax(1.838×10⁻³)和ADCdev(0.148×10⁻³)的最佳临界值。高于临界值的ADCmin与较差的DFS(风险比(HR)= 3.632 - 95%置信区间(CI):1.094 - 12.054;p = 0.035)和DSS(HR = 4.401 - 95% CI:1.048 - 18.483;p = 0.043)显著相关。
在原发肿瘤中测量的治疗前ADCmax可能与FIGO分期和淋巴结状态相关。治疗前ADCmin可能是接受根治性放化疗的宫颈癌患者无病生存期和疾病特异性生存期的一个预后因素。目前正在对这些发现进行前瞻性验证。