Abdel-Wahab Noha, Shah Mohsin, Suarez-Almazor Maria E
Section of Rheumatology and Clinical Immunology, Department of General Internal Medicine, University of Texas MD Anderson Cancer Center, Houston, Texas, United States of America.
Rheumatology and Rehabilitation Department, Assiut University Hospitals, Assiut, Egypt.
PLoS One. 2016 Jul 29;11(7):e0160221. doi: 10.1371/journal.pone.0160221. eCollection 2016.
Three checkpoint inhibitor drugs have been approved by the US Food and Drug Administration for use in specific types of cancers. While the results are promising, severe immunotherapy-related adverse events (irAEs) have been reported.
To conduct a systematic review of case reports describing the occurrence of irAEs in patients with cancer following checkpoint blockade therapy, primarily to identify potentially unrecognized or unusual clinical findings and toxicity.
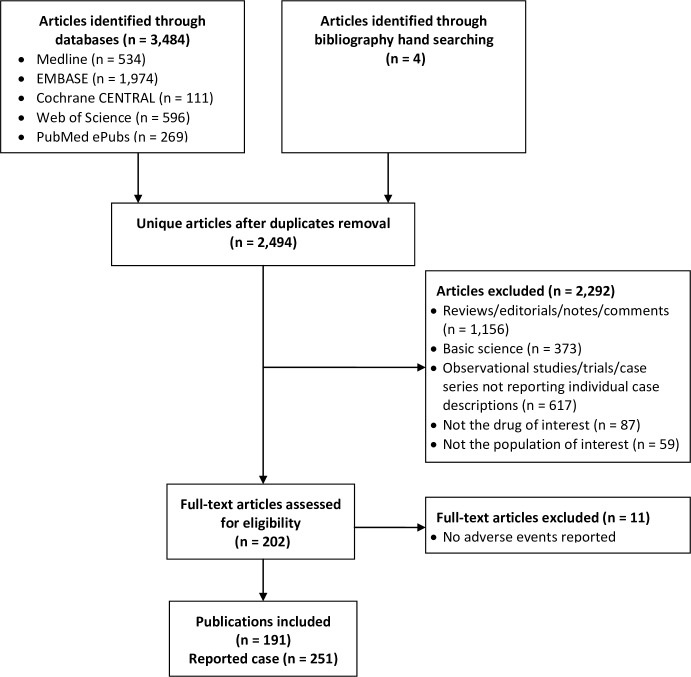
We searched Medline, EMBASE, Web of Science, PubMed ePubs, and Cochrane CENTRAL with no restriction through August 2015.
Studies reporting cases of cancer develop irAEs following treatment with anti CTLA-4 (ipilimumab) or anti PD-1 (nivolumab or pembrolizumab) antibodies were included.
We extracted data on patient characteristics, irAEs characteristics, how irAEs were managed, and their outcomes.
191 publications met inclusion criteria, reporting on 251 cases. Most patients had metastatic melanoma (95.6%), and the majority were treated with ipilimumab (93.2%). Autoimmune colitis, hepatitis, endocrinopathies, and cutaneous irAEs were the most frequently reported irAEs in ipilimumab treated patients. A broad spectrum of toxicities were reported for almost every body system. Moreover, well-defined diseases such as sarcoidosis, polyarthritis, polymyalgia rheumatica/arteritis, lupus, celiac disease, dermatomyositis, and Vogt-Koyanagi-like syndrome were reported. The most frequent irAEs reported with anti-PD1 agents were dermatitis for pembrolizumab, and thyroid disease and pneumonitis for nivolumab. Complete resolution of adverse events occurred in most cases. However, persistent irAEs and death were reported, mainly in patients treated with ipilimumab.
Our study is limited by information available in the original reports.
Evidence from case reports shows that cancer patients develop irAEs following checkpoint blockade therapy, and can occasionally develop clearly defined autoimmune systemic diseases. While discontinuation of therapy and/or treatment can result in resolution of irAEs, long-term sequelae and death have been reported.
三种检查点抑制剂药物已获美国食品药品监督管理局批准用于特定类型的癌症。虽然结果令人鼓舞,但已报告了严重的免疫治疗相关不良事件(irAE)。
对描述癌症患者在检查点阻断治疗后发生irAE的病例报告进行系统评价,主要是为了识别潜在未被认识或不寻常的临床发现及毒性。
我们检索了截至2015年8月的Medline、EMBASE、科学网、PubMed电子出版物和Cochrane CENTRAL,无任何限制。
纳入报告癌症患者在接受抗CTLA-4(伊匹单抗)或抗PD-1(纳武单抗或派姆单抗)抗体治疗后发生irAE的研究。
我们提取了关于患者特征、irAE特征、irAE的处理方式及其结局的数据。
191篇出版物符合纳入标准,报告了251例病例。大多数患者患有转移性黑色素瘤(95.6%),且大多数接受伊匹单抗治疗(93.2%)。自身免疫性结肠炎、肝炎、内分泌病和皮肤irAE是伊匹单抗治疗患者中最常报告的irAE。几乎每个身体系统都报告了广泛的毒性。此外,还报告了明确的疾病,如结节病、多关节炎、风湿性多肌痛/动脉炎、狼疮、乳糜泻、皮肌炎和类Vogt-Koyanagi综合征。抗PD-1药物报告的最常见irAE是派姆单抗引起的皮炎,纳武单抗引起的甲状腺疾病和肺炎。大多数情况下不良事件完全缓解。然而,报告了持续性irAE和死亡,主要发生在接受伊匹单抗治疗的患者中。
我们的研究受原始报告中可用信息的限制。
病例报告的证据表明,癌症患者在检查点阻断治疗后会发生irAE,偶尔会发展为明确的自身免疫性全身性疾病。虽然停止治疗和/或进行治疗可导致irAE缓解,但已报告有长期后遗症和死亡情况。