Konvalinka Ana, Batruch Ihor, Tokar Tomas, Dimitromanolakis Apostolos, Reid Shelby, Song Xuewen, Pei York, Drabovich Andrei P, Diamandis Eleftherios P, Jurisica Igor, Scholey James W
Division of Nephrology, Department of Medicine, Toronto General Hospital, University Health Network, University of Toronto, 11-PMB-189, 585 University Avenue, Toronto, ON M5G 2N2 Canada ; Toronto General Research Institute, University Health Network, Toronto, Canada.
Department of Laboratory Medicine and Pathobiology, Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital, University of Toronto, Toronto, Canada.
Clin Proteomics. 2016 Aug 5;13:16. doi: 10.1186/s12014-016-9117-x. eCollection 2016.
Angiotensin-II (Ang II) mediates progression of autosomal-dominant polycystic kidney disease (ADPKD) and other chronic kidney diseases (CKD). However, markers of kidney Ang II activity are lacking. We previously defined 83 Ang II-regulated proteins in vitro, which reflected kidney Ang II activity in vivo.
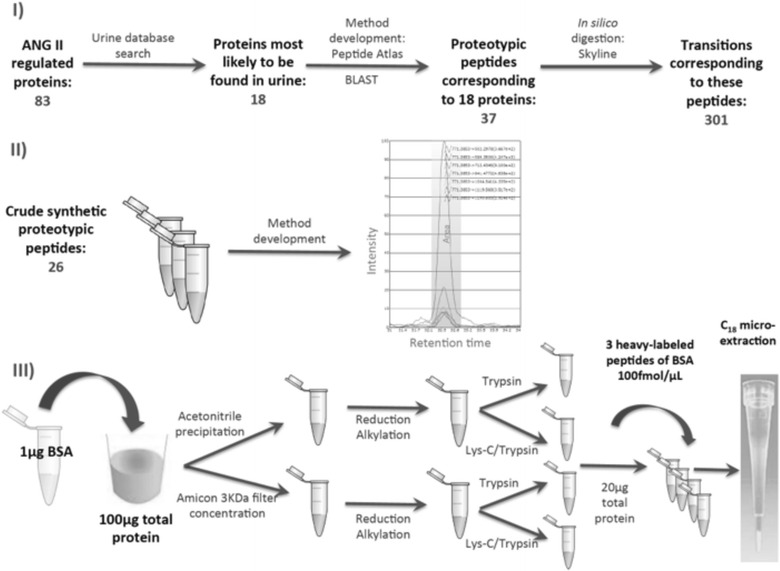
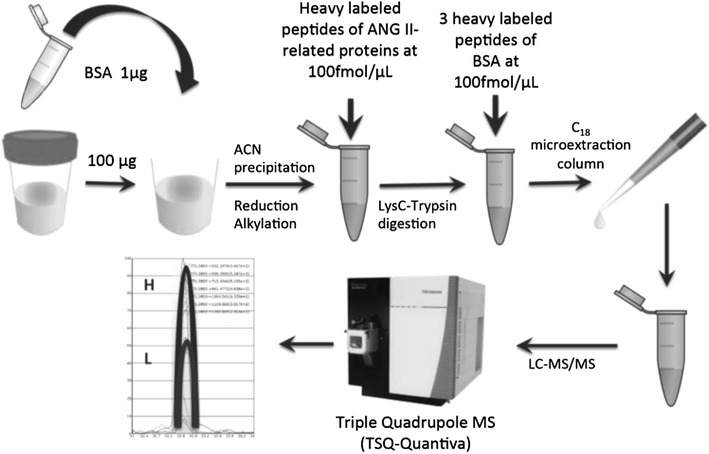
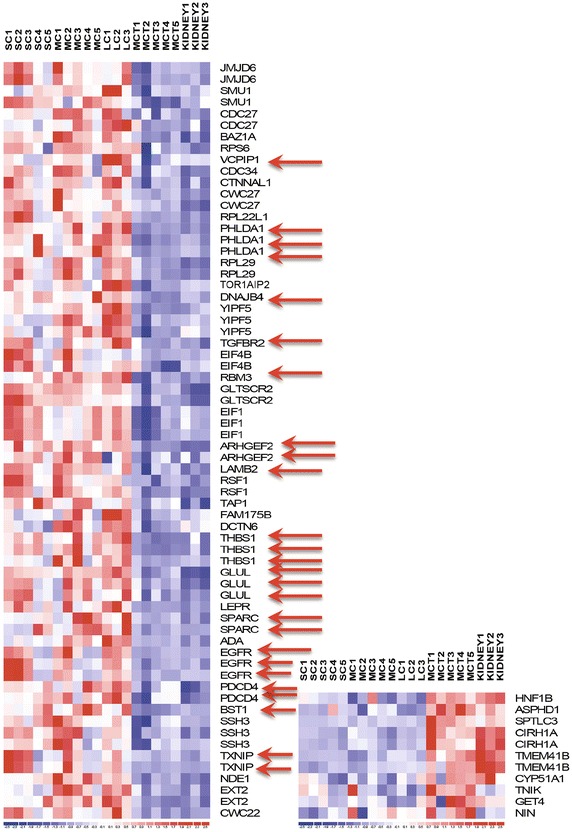
In this study, we developed selected reaction monitoring (SRM) assays for quantification of Ang II-regulated proteins in urine of ADPKD and CKD patients. We demonstrated that 47 of 83 Ang II-regulated transcripts were differentially expressed in cystic compared to normal kidney tissue. We then developed SRM assays for 18 Ang II-regulated proteins overexpressed in cysts and/or secreted in urine. Methods that yielded CV ≤ 6 % for control proteins, and recovery ~100 % were selected. Heavy-labeled peptides corresponding to 13 identified Ang II-regulated peptides were spiked into urine samples of 17 ADPKD patients, 9 patients with CKD predicted to have high kidney Ang II activity and 11 healthy subjects. Samples were then digested and analyzed on triple-quadrupole mass spectrometer in duplicates.
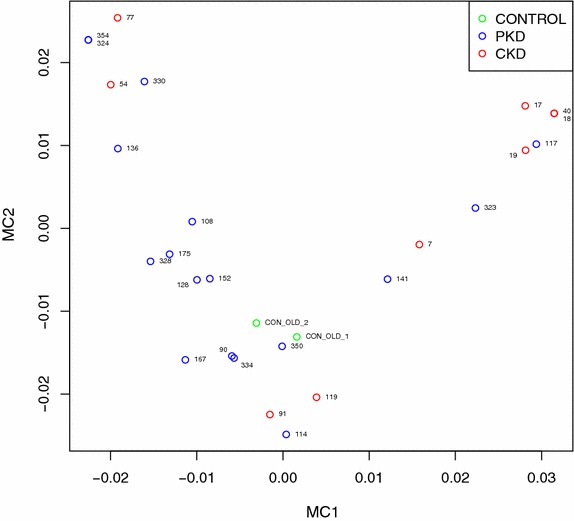
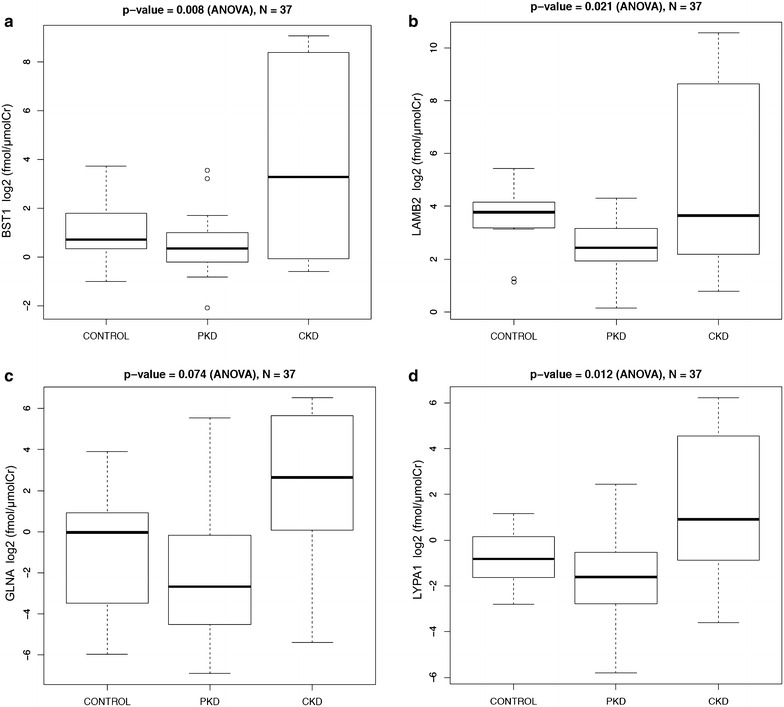
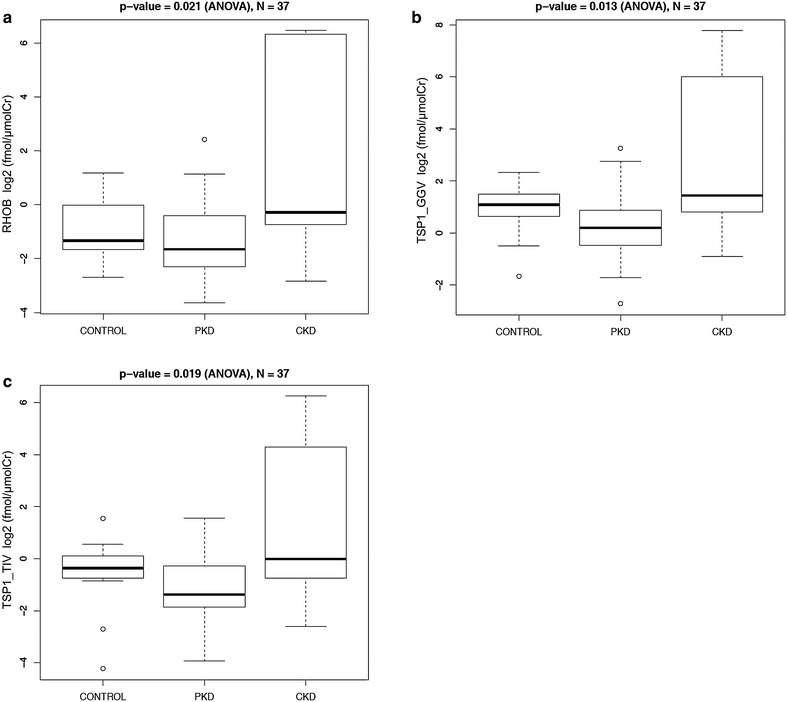
Calibration curves demonstrated linearity (R(2) > 0.99) and within-run CVs < 9 % in the concentration range of 7/13 peptides. Peptide concentrations were normalized by urine creatinine. Deamidated peptide forms were monitored, and accounted for <15 % of the final concentrations. Urine excretion rates of proteins BST1, LAMB2, LYPA1, RHOB and TSP1 were significantly different (p < 0.05, one-way ANOVA) between patients with CKD, those with ADPKD and healthy controls. Urine protein excretion rates were highest in CKD patients and lowest in ADPKD patients. Univariate analysis demonstrated significant association between urine protein excretion rates of most proteins and disease group (p < 0.05, ANOVA) as well as sex (p < 0.05, unpaired t test). Multivariate analysis across protein concentration, age and sex demonstrated good separation between ADPKD and CKD patients.
We have optimized methods for quantification of Ang II-regulated proteins, and we demonstrated that they reflected differences in underlying kidney disease in this pilot study. High urine excretion of Ang II-regulated proteins in CKD patients likely reflects high kidney Ang II activity. Low excretion in ADPKD appears related to lack of communication between cysts and tubules. Future studies will determine whether urine excretion rate of Ang II-regulated proteins correlates with kidney Ang II activity in larger cohorts of chronic kidney disease patients.
血管紧张素II(Ang II)介导常染色体显性遗传性多囊肾病(ADPKD)和其他慢性肾脏病(CKD)的进展。然而,目前尚缺乏反映肾脏Ang II活性的标志物。我们之前在体外鉴定出83种受Ang II调控的蛋白,这些蛋白可反映体内的肾脏Ang II活性。
在本研究中,我们开发了选择性反应监测(SRM)分析法,用于定量检测ADPKD和CKD患者尿液中的Ang II调控蛋白。我们发现,与正常肾组织相比,83种受Ang II调控的转录本中有47种在囊肿组织中差异表达。随后,我们针对18种在囊肿中过表达和/或在尿液中分泌的受Ang II调控蛋白开发了SRM分析法。选择对对照蛋白变异系数(CV)≤6%且回收率约为100%的方法。将与13种已鉴定的受Ang II调控肽段相对应的重标记肽段加入17例ADPKD患者、9例预计肾脏Ang II活性较高的CKD患者和11名健康受试者的尿液样本中。然后对样本进行消化,并在三重四极杆质谱仪上进行重复分析。
校准曲线在7/13种肽段的浓度范围内呈线性(R(2)>0.99),批内CV<9%。肽段浓度通过尿肌酐进行标准化。监测了去酰胺化肽段形式,其占最终浓度的比例<15%。CKD患者、ADPKD患者和健康对照之间,蛋白BST1、LAMB2、LYPA1、RHOB和TSP1的尿排泄率存在显著差异(p<0.05,单因素方差分析)。CKD患者的尿蛋白排泄率最高,ADPKD患者最低。单因素分析显示,大多数蛋白的尿蛋白排泄率与疾病组(p<0.05,方差分析)以及性别(p<0.05,非配对t检验)之间存在显著关联。对蛋白浓度、年龄和性别进行多因素分析显示,ADPKD和CKD患者之间有良好的区分度。
我们优化了定量检测Ang II调控蛋白的方法,并且在本初步研究中证明这些方法可反映潜在肾脏疾病的差异。CKD患者中Ang II调控蛋白的高尿排泄量可能反映了较高的肾脏Ang II活性。ADPKD患者中该蛋白的低排泄量似乎与囊肿和肾小管之间缺乏沟通有关。未来的研究将确定在更大规模的慢性肾脏病患者队列中,Ang II调控蛋白的尿排泄率是否与肾脏Ang II活性相关。