Tandon Puneeta, James Matthew T, Abraldes Juan G, Karvellas Constantine J, Ye Feng, Pannu Neesh
Cirrhosis Care Clinic, Division of Gastroenterology, University of Alberta, Edmonton, Alberta, Canada.
CEGIIR, Department of Medicine, University of Alberta, Edmonton, Alberta, Canada.
PLoS One. 2016 Aug 9;11(8):e0160394. doi: 10.1371/journal.pone.0160394. eCollection 2016.
The implementation of new serum creatinine (SCr)-based criteria for acute kidney injury (AKI) has brought to light several areas of uncertainty in patients with cirrhosis.
Population-based cohort study.
SETTING & PARTICIPANTS: Adults with cirrhosis hospitalized between 2002-2012.
We aimed to address the prognostic implications of the new AKI criteria in cirrhosis.
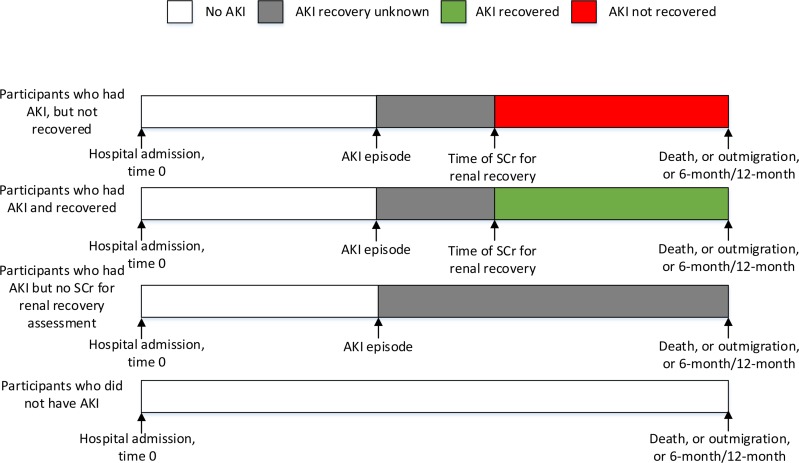
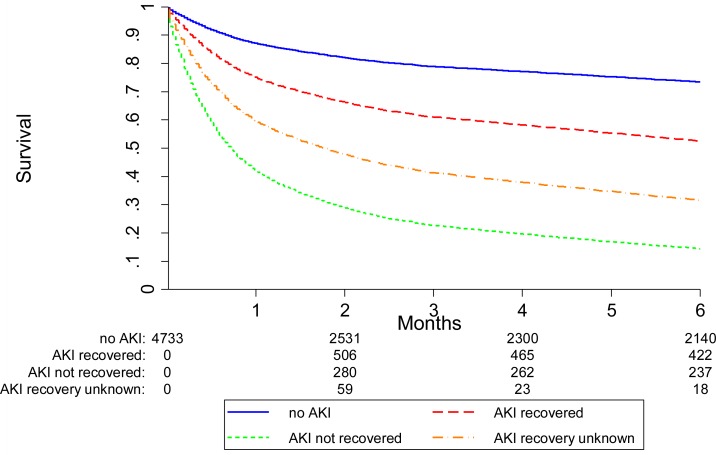
Baseline kidney function was defined from all outpatient SCr within 3 months before hospitalization. Cox proportional hazards models were fit to examine associations between AKI, renal recovery and all-cause mortality.
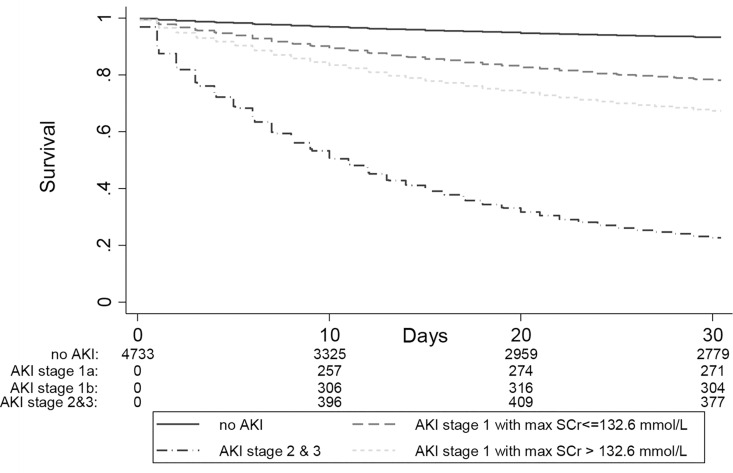
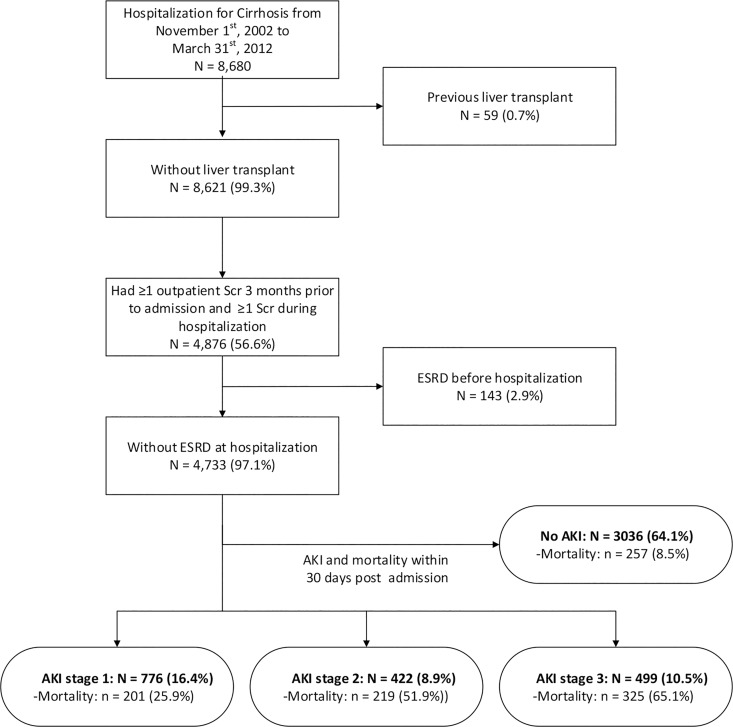
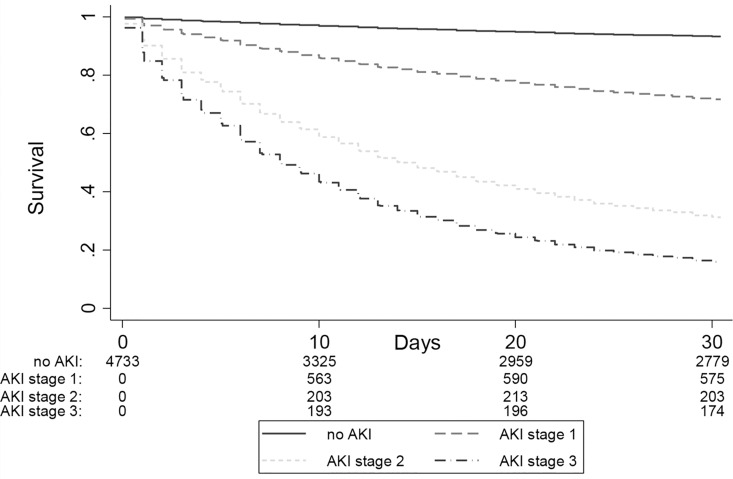
4,733 patients were studied. The 30-day mortality was higher for participants with AKI (43.9% vs 8.5%; p-value<0.001), and increased with AKI severity. The highest incidence of AKI occurred when the lowest SCr within the three months prior to admission was used to define baseline. The hazard ratio for mortality using the lowest SCr within 3 months and the closest pre-admission SCr (definition suggested by the recent consensus guideline) were similar, validating the use of the latter measure. As compared to patients without AKI, stage 1 AKI with maximum SCr ≤132 mmol/L remained associated with a 3.5-fold increased hazard of death at 30 days (95% CI 2.6 to 4.7).
As an observational study, the results were vulnerable to residual confounding and ascertainment bias in the use of laboratory data to identify AKI. We did not have access to liver function or disease etiology variables and were unable to adjust for these in our analyses.
These results confirm the graded relationship between AKI severity, renal recovery, and mortality and further clarify previously discordant reports about the prognostic relevance of new AKI criteria in patients with cirrhosis.
基于血清肌酐(SCr)的急性肾损伤(AKI)新诊断标准的实施揭示了肝硬化患者存在的几个不确定性领域。
基于人群的队列研究。
2002年至2012年间住院的成年肝硬化患者。
我们旨在探讨新的AKI标准对肝硬化患者的预后影响。
住院前3个月内所有门诊SCr定义为基线肾功能。采用Cox比例风险模型来检验AKI、肾功能恢复与全因死亡率之间的关联。
共研究了4733例患者。AKI患者的30天死亡率更高(43.9%对8.5%;p值<0.001),且随AKI严重程度增加。AKI发生率最高的情况是采用入院前三个月内最低的SCr来定义基线。使用入院前三个月内最低的SCr和入院前最近的SCr(近期共识指南建议的定义)计算的死亡风险比相似,验证了后者的实用性。与无AKI的患者相比,最大SCr≤132 mmol/L的1期AKI患者在30天时死亡风险仍增加3.5倍(95%置信区间2.6至4.7)。
作为一项观察性研究,结果容易受到残余混杂因素的影响,以及在使用实验室数据识别AKI时存在的确定偏倚。我们无法获取肝功能或疾病病因变量,且在分析中无法对这些因素进行调整。
这些结果证实了AKI严重程度、肾功能恢复和死亡率之间的分级关系,并进一步阐明了先前关于新的AKI标准对肝硬化患者预后相关性的不一致报道。