Kanias Tamir, Sinchar Derek, Osei-Hwedieh David, Baust Jeffrey J, Jordan Andrew, Zimring James C, Waterman Hayley R, de Wolski Karen S, Acker Jason P, Gladwin Mark T
Pittsburgh Heart, Lung, Blood, and Vascular Medicine Institute, University of Pittsburgh, Pittsburgh, Pennsylvania.
Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania.
Transfusion. 2016 Oct;56(10):2571-2583. doi: 10.1111/trf.13745. Epub 2016 Aug 9.
Red blood cell (RBC) hemolysis represents an intrinsic mechanism for human vascular disease. Intravascular hemolysis releases hemoglobin and other metabolites that inhibit nitric oxide signaling and drive oxidative and inflammatory stress. Although these pathways are important in disease pathogenesis, genetic and population modifiers of hemolysis, including sex, have not been established.
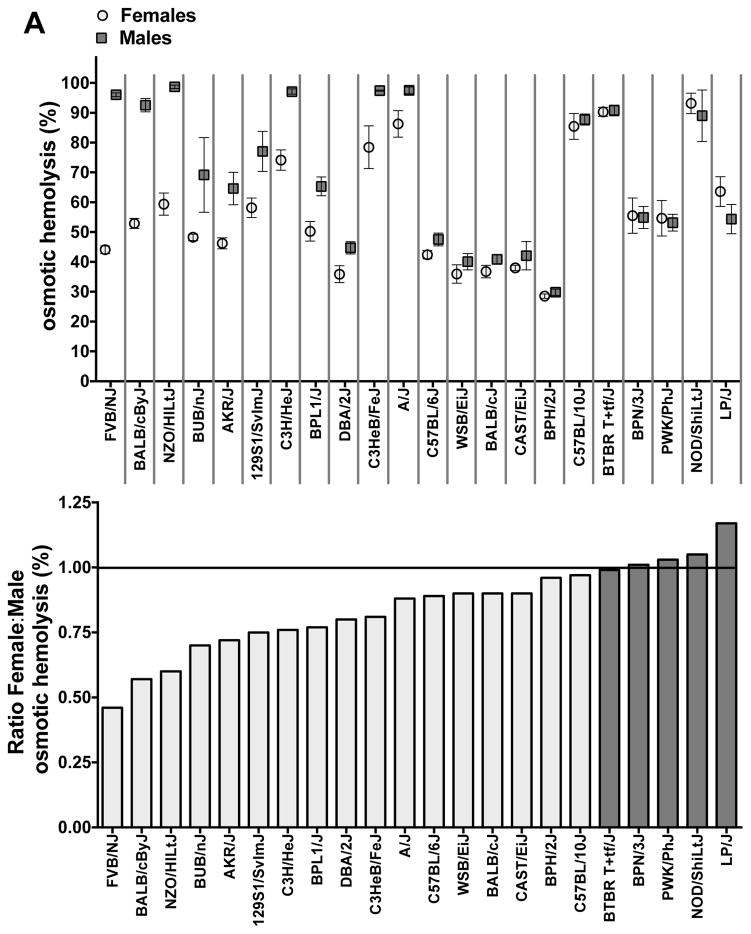
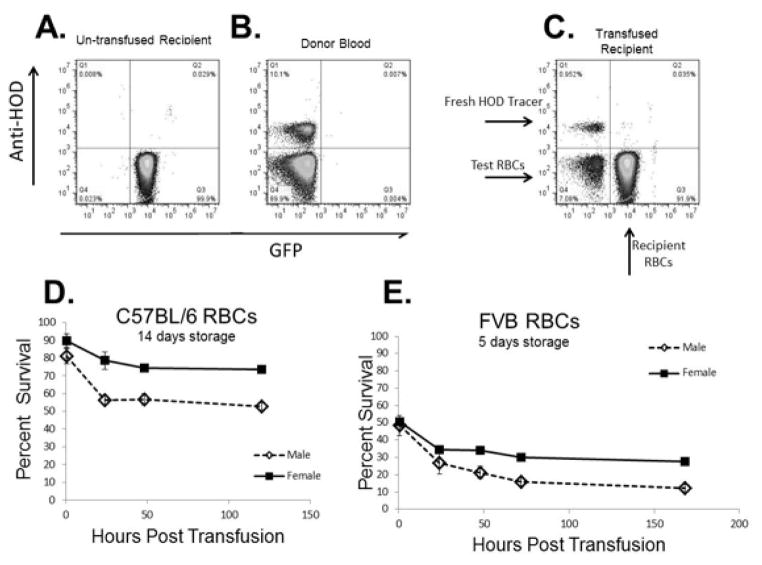
We studied sex differences in storage or stress-induced hemolysis in RBC units from the United States and Canada in 22 inbred mouse strains and in patients with sickle cell disease (SCD) using measures of hemolysis in 315 patients who had homozygous SS hemoglobin from the Walk-PHASST cohort. A mouse model also was used to evaluate posttransfusion recovery of stored RBCs, and gonadectomy was used to determine the mechanisms related to sex hormones.
An analysis of predisposition to hemolysis based on sex revealed that male RBCs consistently exhibit increased susceptibility to hemolysis compared with females in response to routine cold storage, under osmotic or oxidative stress, after transfusion in mice, and in patients with SCD. The sex difference is intrinsic to the RBC and is not mediated by plasmatic factors or female sex hormones. Importantly, orchiectomy in mice improves RBC storage stability and posttransfusion recovery, whereas testosterone repletion therapy exacerbates hemolytic response to osmotic or oxidative stress.
Our findings suggest that testosterone increases susceptibility to hemolysis across human diseases, suggesting that male sex may modulate clinical outcomes in blood storage and SCD and establishing a role for donor genetic variables in the viability of stored RBCs and in human hemolytic diseases.
红细胞溶血是人类血管疾病的一种内在机制。血管内溶血会释放血红蛋白和其他代谢产物,这些产物会抑制一氧化氮信号传导,并引发氧化应激和炎症应激。尽管这些途径在疾病发病机制中很重要,但溶血的遗传和人群修饰因素,包括性别,尚未明确。
我们使用来自Walk-PHASST队列的315例纯合子SS血红蛋白患者的溶血指标,研究了美国和加拿大22种近交小鼠品系以及镰状细胞病(SCD)患者的红细胞单位在储存或应激诱导的溶血中的性别差异。还使用小鼠模型评估储存红细胞的输血后恢复情况,并通过去势手术来确定与性激素相关的机制。
基于性别的溶血易感性分析显示,在常规冷藏、渗透压或氧化应激、小鼠输血后以及SCD患者中,与雌性相比,雄性红细胞对溶血的易感性始终增加。这种性别差异是红细胞固有的,不受血浆因子或女性性激素介导。重要的是,小鼠去势可改善红细胞储存稳定性和输血后恢复情况,而睾酮补充疗法会加剧对渗透压或氧化应激的溶血反应。
我们的研究结果表明,睾酮会增加人类疾病中对溶血的易感性,这表明男性性别可能会调节血液储存和SCD的临床结果,并确定供体遗传变量在储存红细胞活力和人类溶血性疾病中的作用。