Zhang Zhen-Yu, Luo Qi-Feng, Yin Xiao-Wei, Dai Zhen-Ling, Basnet Shiva, Ge Hai-Yan
Department of Gastrointestinal Surgery, Shanghai East Hospital, Tongji University School of Medicine, Pudong New District, No. 150, Jimo Road, Shanghai, 200120, China.
Department of General Surgery, Qingpu Branch of Zhongshan Hospital, Fudan University, Shanghai, China.
BMC Cancer. 2016 Aug 19;16(1):658. doi: 10.1186/s12885-016-2684-4.
The predictive accuracy of the American Joint Committee on Cancer (AJCC) stages of colorectal cancer (CRC) is mediocre. This study aimed to develop postoperative nomograms to predict cancer-specific survival (CSS) and overall survival (OS) after CRC resection without preoperative therapy.
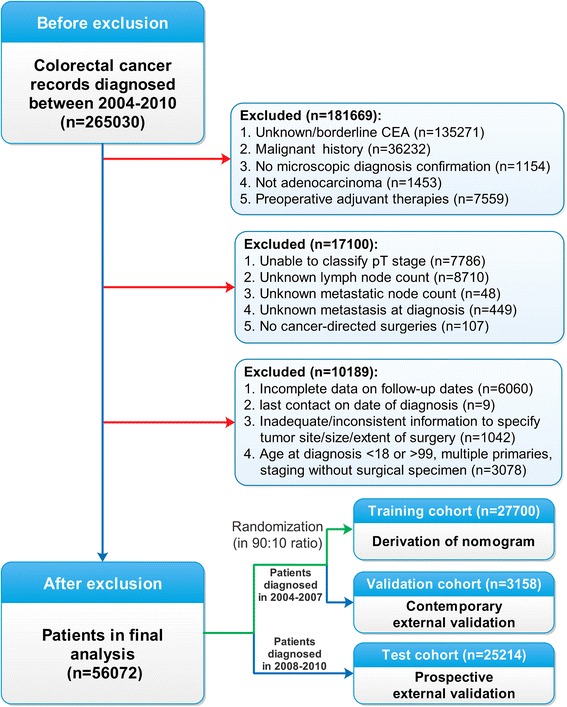
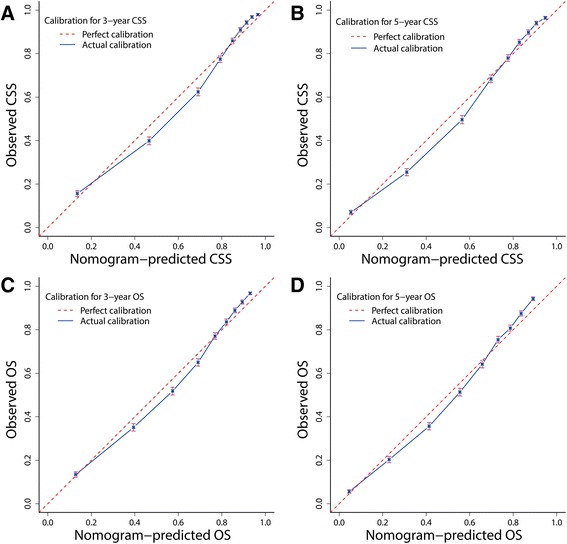
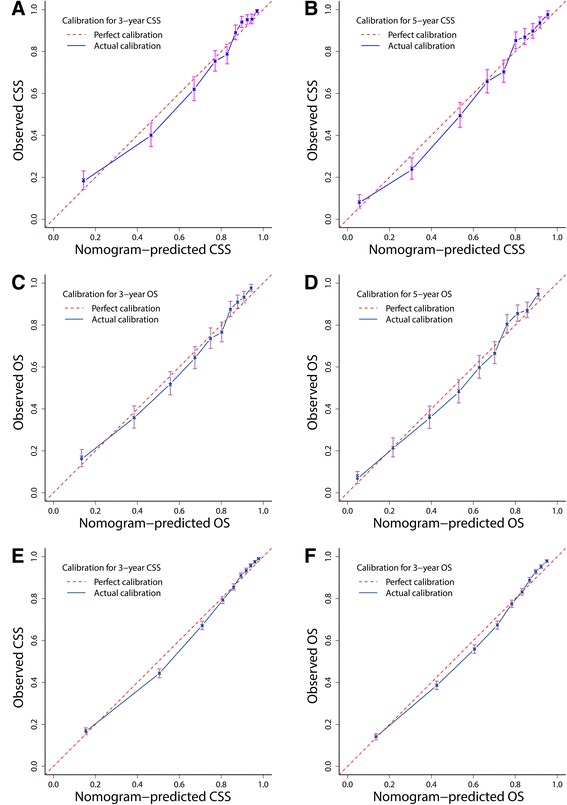
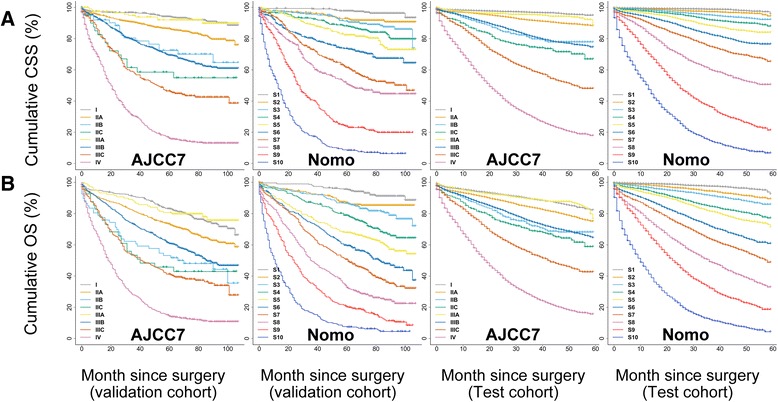
Eligible patients with stage I to IV CRC (n = 56072) diagnosed from 2004 to 2010 were selected from the Surveillance, Epidemiology, and End Results (SEER) database. The patients were allocated into training (n = 27,700), contemporary (n = 3158), and prospective (n = 25,214) validation cohorts. Clinically important variables were incorporated and selected using the Akaike information criterion in multivariate Cox regressions to derive nomograms with the training cohort. The performance of the nomograms was assessed and externally testified using the concordance index (c-index), bootstrap validation, calibration, time-dependent receiver-operating characteristic curves, Kaplan-Meier curves, mosaic plots, and decision curve analysis (DCA). Performance of the conventional AJCC stages was also compared with the nomograms using similar statistics.
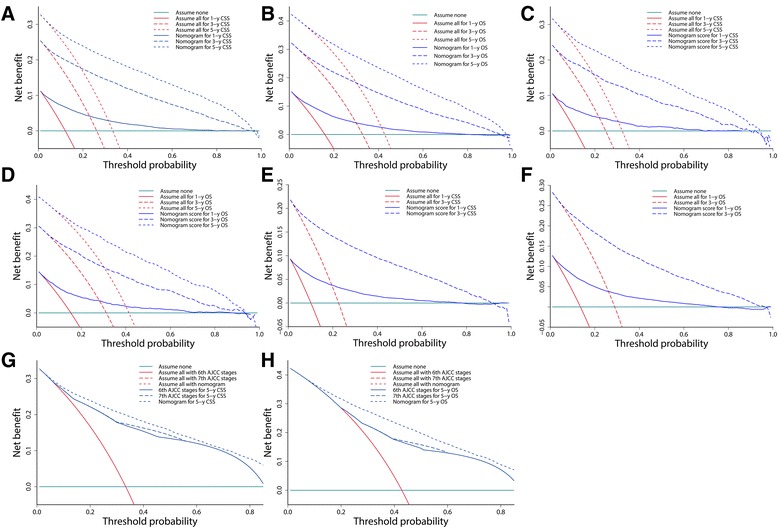
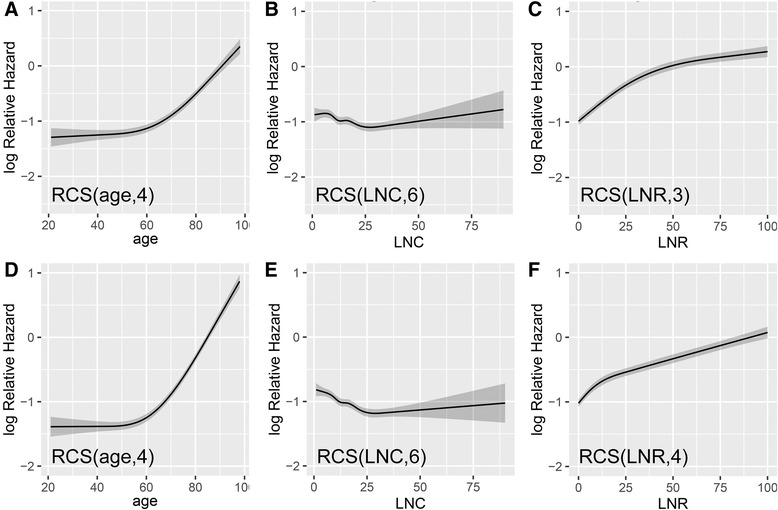
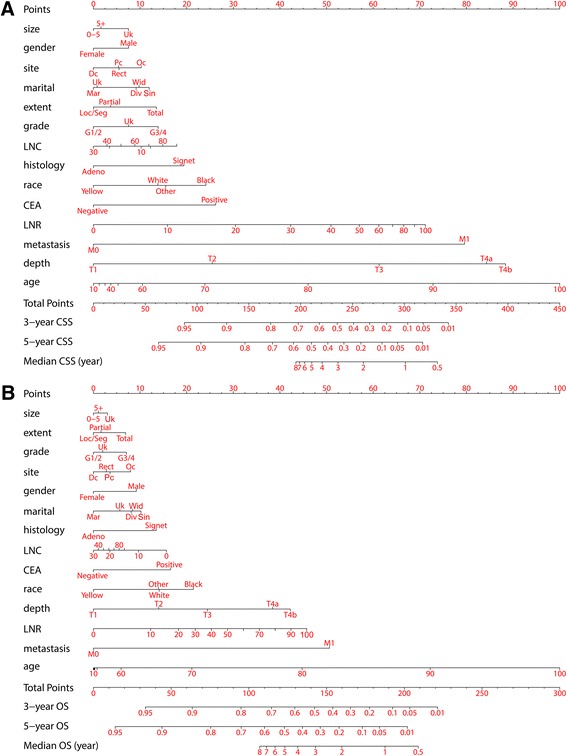
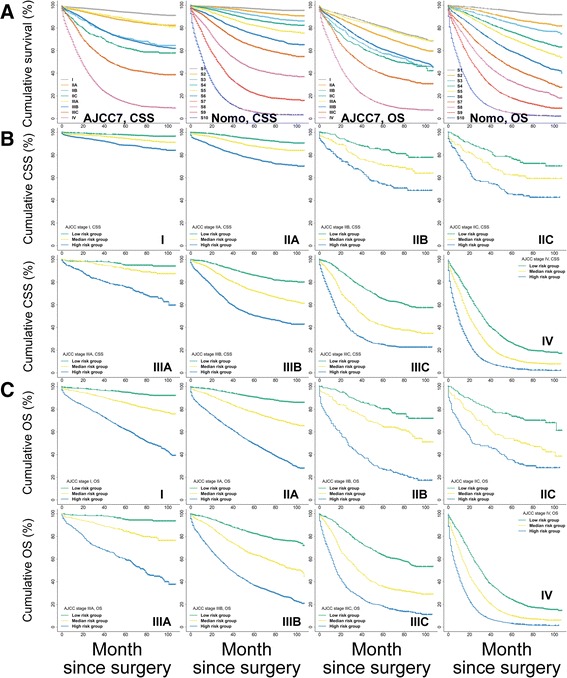
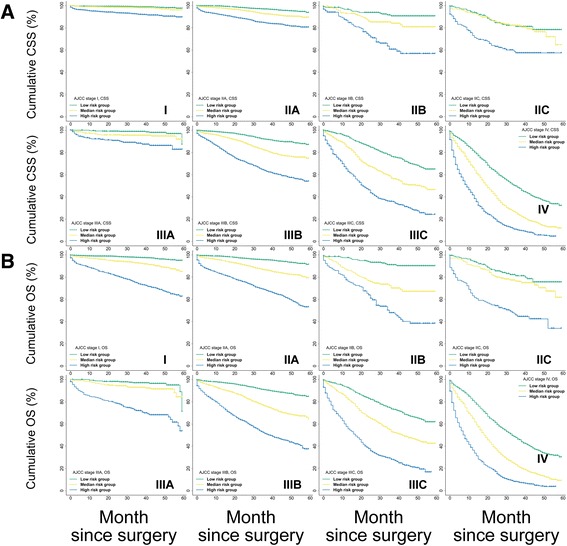
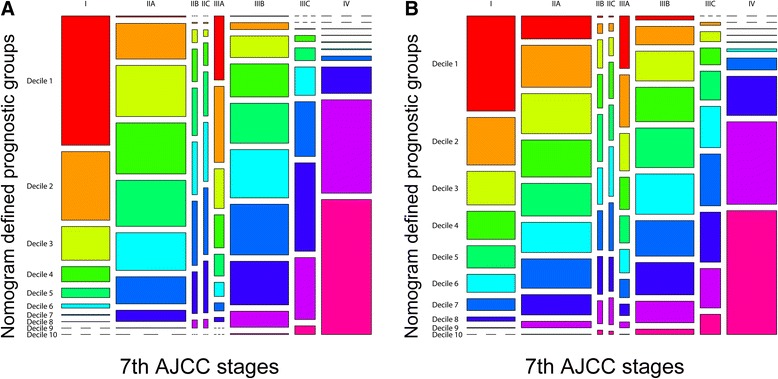
The nomograms for CSS and OS shared common predictors: sex, age, race, marital status, preoperative carcinoembryonic antigen status, surgical extent, tumor size, location, histology, differentiation, infiltration depth, lymph node count, lymph node ratio, and metastasis. The c-indexes of the nomograms for CSS and OS were 0.816 (95 % CI 0.810-0.822) and 0.777 (95 % CI 0.772-0.782), respectively. Performance evaluations showed that the nomograms achieved considerable predictive accuracy, appreciable reliability, and significant clinical validity with wide practical threshold probabilities, while the results remained reproducible when applied to the validation cohorts. Additionally, model comparisons and DCA proved that the nomograms excelled in stratifying each AJCC stage into three significant prognostic subgroups, allowing for more robust risk classification with an improved net benefit.
We propose two prognostic nomograms that exhibit improved predictive accuracy and net benefit for patients who have undergone CRC resection. The established nomograms are intended for risk assessment and selection of suitable patients who may benefit from adjuvant therapy and intensified follow-up after surgery. Independent external validations may still be required.
美国癌症联合委员会(AJCC)结直肠癌(CRC)分期的预测准确性一般。本研究旨在开发术后列线图,以预测未经术前治疗的CRC切除术后的癌症特异性生存(CSS)和总生存(OS)。
从监测、流行病学和最终结果(SEER)数据库中选取2004年至2010年诊断为I至IV期CRC的符合条件患者(n = 56072)。将患者分为训练队列(n = 27700)、当代队列(n = 3158)和前瞻性队列(n = 25214)进行验证。在多变量Cox回归中使用赤池信息准则纳入并选择临床重要变量,以从训练队列中得出列线图。使用一致性指数(c指数)、自助法验证、校准、时间依赖性受试者操作特征曲线、Kaplan-Meier曲线、镶嵌图和决策曲线分析(DCA)评估列线图的性能并进行外部验证。还使用类似统计方法将传统AJCC分期的性能与列线图进行比较。
CSS和OS的列线图共有共同的预测因素:性别、年龄、种族、婚姻状况、术前癌胚抗原状态、手术范围、肿瘤大小、位置、组织学、分化程度、浸润深度、淋巴结计数、淋巴结比率和转移情况。CSS和OS列线图的c指数分别为0.816(95%CI 0.810 - 0.822)和0.777(95%CI 0.772 - 0.782)。性能评估表明,列线图具有相当高的预测准确性、可观的可靠性和显著的临床有效性,且具有广泛的实用阈值概率,同时应用于验证队列时结果仍具有可重复性。此外,模型比较和DCA证明,列线图在将每个AJCC分期分为三个显著的预后亚组方面表现出色,能够进行更稳健的风险分类并提高净效益。
我们提出了两个预后列线图,它们对接受CRC切除的患者具有更高的预测准确性和净效益。所建立的列线图旨在进行风险评估,并选择可能从辅助治疗和术后强化随访中获益的合适患者。可能仍需要独立的外部验证。