Kobayashi Kenya, Matsumoto Fumihiko, Kodaira Makoto, Mori Taisuke, Murakami Naoya, Yoshida Akihiko, Maki Daisuke, Teshima Masanori, Fukasawa Masahiko, Itami Jun, Asai Masahiro, Yoshimoto Seiichi
Department of Head and Neck Oncology, National Cancer Center Hospital, Tokyo, Japan.
Department of Medical Oncology and Breast Oncology, National Cancer Center Hospital, Tokyo, Japan.
Cancer Med. 2016 Oct;5(10):2708-2714. doi: 10.1002/cam4.855. Epub 2016 Aug 26.
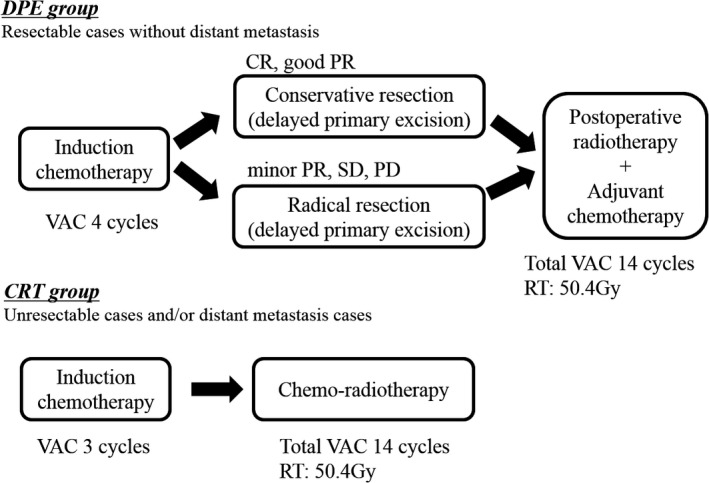
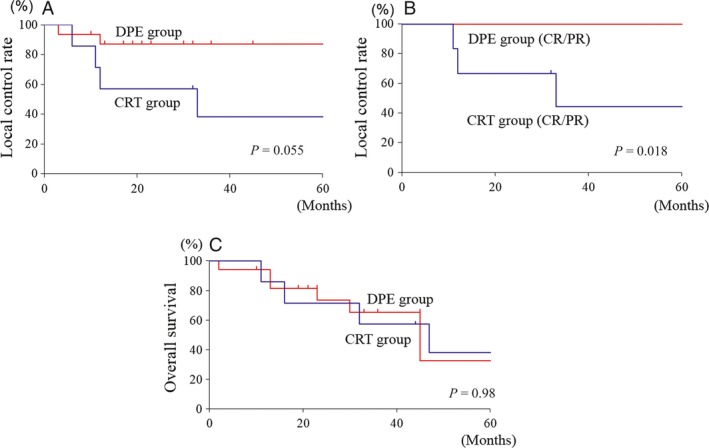
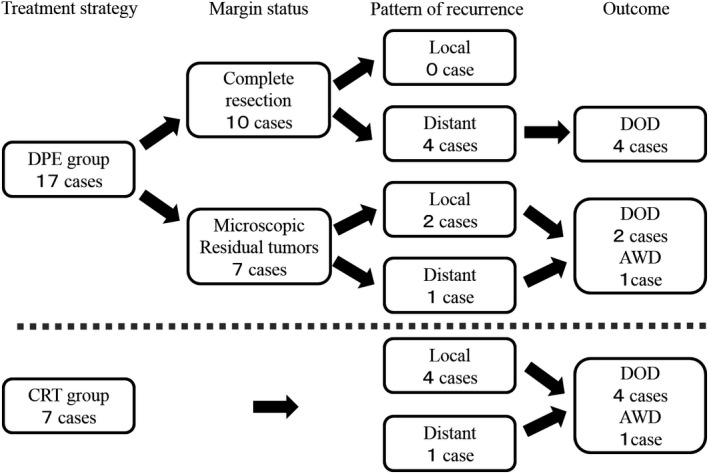
Adult rhabdomyosarcoma (RMS) is a highly aggressive tumor. Multidisciplinary treatment is important. However, the role of surgery is controversial. The purpose of this study was to reveal the role of a delayed primary excision (DPE) after induction chemotherapy (IC) in localized nonmetastatic adult head and neck RMS. We retrospectively reviewed 24 adult head and neck RMS. Treatment was classified into the following two groups: the DPE group, who received IC followed by surgery, postoperative radiotherapy, and adjuvant chemotherapy (17 patients); the chemoradiotherapy (CRT) group, who received IC followed by chemoradiotherapy (seven patients). We analyzed the efficacy of IC, local control rate (LCR), and overall survival (OS). In the DPE group, 10 patients (59%) underwent complete surgical resection. In the evaluation of the surgical specimens, 14 patients (82%) had residual viable tumors after IC. The response to IC was significantly associated with the 3-year LCR (CR/PR vs.
SD/PD: 100% vs. 33%, P = 0.0014). In patients with good response to chemotherapy, the DPE group had a significantly better 3-year LCR compared with that of the CRT group (DPE group vs. CRT group, 100% vs. 44%, P = 0.018). However, the treatment modalities were not associated with OS (DPE group vs. CRT group, 65% vs. 57%: P = 0.98). The recurrence patterns differed according to treatments, and distant metastases were more frequent in the DPE group. DPE may impact local control of localized nonmetastatic adult head and neck RMS. Poor response to IC is a risk factor for local recurrence.
成人横纹肌肉瘤(RMS)是一种侵袭性很强的肿瘤。多学科治疗很重要。然而,手术的作用存在争议。本研究的目的是揭示诱导化疗(IC)后延迟一期切除(DPE)在局限性非转移性成人头颈部RMS中的作用。我们回顾性分析了24例成人头颈部RMS患者。治疗分为以下两组:DPE组,接受IC后行手术、术后放疗及辅助化疗(17例患者);放化疗(CRT)组,接受IC后行放化疗(7例患者)。我们分析了IC的疗效、局部控制率(LCR)和总生存期(OS)。在DPE组,10例患者(59%)接受了完整的手术切除。在对手术标本的评估中,14例患者(82%)在IC后有残留的存活肿瘤。IC的反应与3年LCR显著相关(CR/PR与SD/PD:100%对33%,P = 0.0014)。在对化疗反应良好的患者中,DPE组的3年LCR明显优于CRT组(DPE组对CRT组,100%对44%,P = 0.018)。然而,治疗方式与OS无关(DPE组对CRT组,65%对57%:P = 0.98)。复发模式因治疗而异,远处转移在DPE组更常见。DPE可能影响局限性非转移性成人头颈部RMS的局部控制。对IC反应不佳是局部复发的危险因素。